[ed. note: Michael Jorrin, who I like to call Doc Gumshoe, is a longtime medical writer (not a doctor) who writes about non-financial health and medical issues for us a couple times a month. Like all of our authors, he chooses his own topics and his words and opinions are his alone. Enjoy!]
While working on the previous Doc Gumshoe installment about Dr Bereliani and his weapon against the Evil Cardiac Killer, I was struck by the large amount of stuff I ran across about diets of one sort or another. I was going to say “information” rather than “stuff” in that preceding sentence because it sounded more respectful and professional. But “information” implies, somehow, that the material is mostly fact-based, and, while the diet manifestos all included a certain quota of facts, they also all skated a good deal beyond the edges of the fact base and onto the thin ice of fashionable conjecture.
I should not have been surprised at the differences among these many diets – after all, some were pure and simple weight-loss diets, while others seemed to be tailored to avoiding specific diseases or conditions. But it got me to thinking that perhaps those differences are more a matter of marketing than of real, legitimate differences in the objectives of the diet. It struck me that it is more likely than not that the person who wants to lose weight also wants to avoid heart disease, stroke, diabetes, cancer, rheumatoid arthritis – indeed, everything from Alzheimer’s disease to Zollinger-Ellison syndrome. Most diseases and conditions in some way relate to metabolism, and changing our diets is a direct way of tinkering with our metabolism. I also got to wondering what the word “diet” really, fundamentally means.
So I consulted my OED. “Diet” is in Volume 4, Creel – Duzepere, and the etymology is unsurprising – from Latin diæta (Greek δίαιτα) meaning “mode of life.” The OED refrains from stating the obvious, which is that diæta is related to the word for day (die). In mediaeval Latin, diæta meant “a day’s journey,” and “diet” also means a meeting of an official assembly of some sort, like the Diet of Worms that we all jested about in 10th grade.
The OED gives fourteen separate definitions for the noun “diet” as well as six more for the verb. Here are the first three for the noun:
- Course of life, way of living of thinking
- Customary course of living as to food; way of feeding
- Prescribed course of food, restricted in kind or limited in quantity, esp. for medical or penal reasons; regimen
The earliest citation in the OED is from Chaucer, “No deyntee morsel passed thrugh hir throte,… Attempree diete was al hir phisik.”
There we have it. “Attempree” by the way means “tempered” or “moderate,” so back in 1386 it was already thought by some that all that was needed for health was a moderate diet. Have we come much farther than that in 630 years?
Looking at those OED definitions, please notice the fundamental distinction between the first two, which characterize the diet as “customary,” and the third, in which the diet is “prescribed.” The diets that we hear and read about are mostly in the second category, but there’s an expectation among the proponents of these diets that they will shift, over time, from being prescribed to being customary.
The unfortunate reality is that, especially for the multitude of weight-loss diets, this almost never happens. Prescribed diets, whether as an avenue to weight loss or to lowering cholesterol levels or to reducing cardiovascular risk, are, for most people, a severe disappointment. People tend to stick to weight-loss diets for about as long as they keep their New Year’s resolutions. Many famous diets of yesteryear have been consigned to the dustbin of history. Diabetics are supposed to keep away from food and drink that carries a high sugar load, but lots of diabetics – once they have started taking their antidiabetic medications – relapse into their former habits.
Current diet apostles recognize this reality and try to craft their diets in such a way that the transition from “prescribed” to “customary” happens a bit more often, for a few more people. They too would like to be able to present their “tempered” diets as the only medicine most people need. To this end, a common feature of the up-to-date diet is that there is no need, ever, for the dieter to feel hungry. If you Google the phrase “stop counting calories,” you get well over 800,000 hits.
One of the recent best-selling diet books is David Ludwig’s Always Hungry?, which hit number three on the New York Times’ how-to- best seller list. According to Ludwig, we can just say goodbye to counting calories. And among other features of his plan, Ludwig advocates as much full-fat yoghurt and as many nuts as you can stuff into yourself. That’s not his whole plan, of course; there are other, less attention-grabbing parts. Ludwig is on the faculty at the Harvard Medical School and a pediatric endocrinologist. Ped endos are the clan of physicians that study and treat diabetes in children and adolescents, and, as such, they are keenly attuned to the effects of food on our metabolism, which is what the whole dieting thing is about. But Ludwig, like other diet proponents, has to put his recommendations in a context that makes it likely that they will be accepted by the populace.
What do the recent crop of diets have in common?
Over time, there has been a shift away from the emphasis on avoiding foods with heavy concentrations of saturated fats and cholesterol. The old-time rogues gallery – especially eggs, butter, and red meat – have been moved out of the cross-hairs. Their places have been taken by added sugars and refined carbohydrates as well as trans-fats.
There are sound reasons for this de-emphasis, although in my view what is logically called for is a moderate change in the course rather than a screeching halt and a reversal of direction. As I wrote in the previous post, severe restrictions on cholesterol intake were based, entirely reasonably at that time, on the discovery that cholesterol was the prime component of the plaque in our arteries. Later discoveries that we ourselves made at least three-quarters of all the cholesterol in our bodies reduced some of the emphasis on dietary cholesterol as the culprit.
Reduced, but not totally exonerated. In spite of the evidence pointing to other things we eat that contribute to the formation of the LDL cholesterol particles that are most implicated in the formation of atherosclerotic plaque, there is some evidence for the participation of dietary cholesterol in the pathology. Specifically, the drug ezetimibe (Zetia, Merck), whose mechanism of action in reducing cholesterol is totally different from either the statins or the PCSK9 inhibitors, needs to be considered. Ezetimibe inhibits the transport of dietary cholesterol from the GI tract into the circulatory system. It does not affect the synthesis of cholesterol at all; its effect is solely on the cholesterol that is in the food we eat – that rogues’ gallery of eggs, butter, and red meat.
In February of this year, we learned that the combination of ezetimibe and simvastatin reduced cardiovascular events such as heart attacks and strokes by about 9% compared with simvastatin alone. We already know that simvastatin, along with other statins, confers a considerable degree of risk reduction. There have been many, many studies, enrolling different types of patients with varying degrees of risk factors, and the results in terms of percentage of risk reduction have varied hugely, but I feel reasonably confident is saying that statin treatment over the long term reduces cardiovascular risk by about 30%. The National Cholesterol Educational Program (NCEP) has, in part, based its treatment guidelines on data showing that a 30 mg/dL reduction in LDL cholesterol reduces the incidence of cardiac events by 30%. So an additional 9% risk reduction, by blocking the absorption of dietary cholesterol, is not negligible.
To put it another way, many current diets are characterized by a huge shift in emphasis: stay away from bread, they preach, but eat as much butter as you want. To which I say, “not so fast.” The tempered diet has room for both.
Does greater emphasis on HDL-cholesterol make sense?
The importance of HDL-cholesterol has been recognized for a long time. The Framingham Risk Calculator subtracts one point from the overall risk score when a person’s HDL level is 60 mg/dL or above, adds one point if it’s between 40 and 49 mg/dL, and adds two points if it’s below 40 mg/dL. The previous Doc Gumshoe piece about the notorious Cardiac Killer explained in some detail the relationship between HDL and cholesterol transport. Let it be enough to say for now that a healthy HDL level – 50 mg/dL or more – is an indication that overall cholesterol transport, in and out, is functioning well.
However, HDL-cholesterol appears to have another beneficial function, namely that it protects the endothelial cells in the vascular system. The endothelial cells form the interior lining of the blood vessels, and one particular component of HDL, apolipoprotein A-1, helps to prevent certain white blood cells called monocytes from attaching to the arterial wall. Those white blood cells are participants in the process of vulnerable plaque formation that results in the release of blood clots and atherosclerotic plaque particles into the blood stream, causing strokes and heart attacks. HDL-cholesterol, it is thought, helps to prevent this process.
Many current popular diet plans include features intended to increase HDL-cholesterol levels. The nuts favored by David Ludwig contain unsaturated fats that favor the increase in HDL cholesterol. Unsaturated fats, both mono- and poly-, are also present in many kinds of fish such as salmon, sardines, herring, mackerel, and sea bass. And they are found in flaxseed, some beans, soy products, and even some green vegetables. Of course, olive oil is the unsaturated fat par excellence and is a featured player in the Mediterranean diet.
The Mediterranean diet tends to be a “customary” diet rather than a “prescribed” diet, and study in Spain confirmed that people who followed the Mediterranean diet as a usual daily practice had a lower incidence of cardiac events than people who were on a prescribed diet emphasizing fruits, vegetables, and minimizing fats of any kind – more like the “food pyramid” diets and diets put forward by the American Heart Association. Also, a study conducted under the Nurses’ Study program found that the Mediterranean diet was associated with longer telomeres. Telomeres protect our DNA, and longer telomeres should lead to increased longevity; therefore the Mediterranean diet might favor increased longevity.
An eminent spokesman for the Mediterranean diet is Dariush Mozaffarian of the Harvard School of Public Health. In a lengthy paper in Circulation (2011;123:2870-2891), he spells out the Mediterranean diet in some detail. For example, his classification of grains is shown in the figure below. The green area at the top is good for us, but as we go down to the dark pink area, the foods on it are on the “be careful” list, and the deep red at the bottom is to be shunned at all costs. However, what Mozaffarian is putting together is a prescribed diet meant to guard against cardiovascular risk. I don’t see Mozaffarian’s presentation of the cardioprotective diet as a customary diet. It’s a bit difficult to imagine that most people who are not specifically concerned with cardiovascular risk would adhere to a customary diet that omitted foods like white bread, pasta, potatoes, corn, and virtually all deserts, as in the figure below.
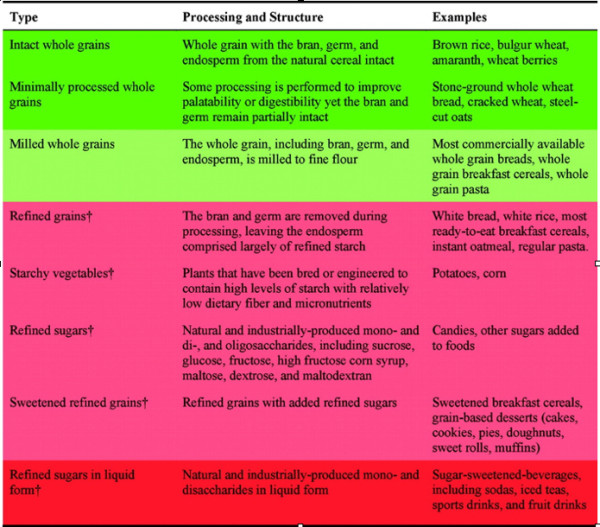
Another diet guru, Gary Taubes, author of Good Calories, Bad Calories, objects to some of the items in the light green area in the table above, namely milled whole grains, which includes those supposedly healthful whole grain breads, breakfast cereals, and pastas. According to Taubes, and to another diet authority, Robert Lustig (not to be confused with David Ludwig!), when those whole grains are milled they get so pulverized that they’re just as bad as refined grains. They claim that this leads to the overproduction of insulin, which in turn instructs the liver to store glucose as fat.
"reveal" emails? If not,
just click here...
So, if we omit milled whole grains, what’s left? And also, how is it that insulin could be bad for us? Isn’t diabetes a disease of insulin deficiency?
Training the dietary cross-hairs on foods with a high glycemic load
The glycemic index quantifies the glucose content of a food or beverage on a scale of 1 to 100, while glycemic load assesses the amount of glucose per serving of that food or beverage. Those data are crucial for constructing a diet, whether a weight-loss diet or a diet aimed at controlling diabetes or reducing cardiovascular risk. At the risk of being tediously repetitive, here’s why:
- Glucose that is not converted to energy tends to be stored as fat.
- Glucose in the bloodstream signals our pancreatic beta cells to secrete insulin, but excessive amounts of insulin can effectively exhaust insulin receptors throughout the body, leading to diabetes.
- Diabetes itself contributes to acute cardiovascular events. Atherosclerotic plaques in persons with diabetes are more unstable and likely to rupture; they contain a richer lipid core and are more susceptible to inflammation.
The shift in emphasis from avoiding high-fat foods to minimizing those that carry a high glycemic load appears to be reasonable. Here’s a short selection from a list of more than 100 food and drink items from the Harvard Medical School:
| Food / beverage | Glycemic index (glucose = 100) | Glycemic load per serving |
| Vanilla cake from Betty Crocker mix | 42 | 24 |
| Bagel, plain white | 72 | 25 |
| Baguette, white | 95 | 15 |
| Coca Cola | 63 | 16 |
| Unsweetened orange juice | 50 | 12 |
| Cornflakes | 93 | 23 |
| Instant oat meal | 83 | 30 |
| Corn on the cob | 60 | 20 |
| Couscous | 65 | 9 |
| White rice | 89 | 43 |
| Milk, full fat | 41 | 5 |
| Milk, skim | 32 | 4 |
| Apple | 39 | 6 |
| Raisins | 64 | 28 |
| Kraft mac & cheese | 64 | 32 |
| Baked russet potato | 111 | 33 |
| Carrots | 35 | 2 |
| Hummus (chick pea dip) | 6 | 0 |
Something that the table makes clear is that it doesn’t matter a whole lot whether the glycemic load is in the form of sugar or refined carbohydrates. That’s because we convert the carbohydrate to glucose really, really quickly. A lot of the difference in glycemic load is, of course, the serving size. For example, the Coca Cola serving is 250 ml, which is about a cup; people who buy those supersized soda pops that Mayor Mike Bloomberg excoriated take in a multiple of that glycemic load. But it’s eye-opening that for equivalent quantities, Coke has three times the glycemic load as whole milk. A quart of Coke carries a glycemic load equivalent to two large baked potatoes.
The glycemic index/load data don’t take into account another bit of data that can have an important impact
on how diet affects our metabolism. Mozaffarian points out an interesting difference between glucose and fructose, fructose being the naturally-occurring form of sugar in most fruits. Fructose produces a somewhat smaller glycemic response, but seems to trigger more lipogenesis – i.e., conversion to fat – than glucose. It has also been suggested that we humans respond somewhat differently to the taste of fructose than to that of sucrose (i.e., sugar). The taste of sugar strikes us as just a bit sweeter. Therefore, to get the equivalent sensation of sweetness, the quantity of fructose (as in high fructose corn syrup, used to sweeten most soda pop) would have to be boosted. But the soda pop makers are reluctant to do that; they probably don’t want to be accused of super-sweetening their products. Therefore, I suspect, many people are simply not satisfied with the old-time 8 ounce soda; thus the supersized containers – and the soda pop makers are okay with that.
Another factor that needs to be considered when thinking about diets is the how they affect our sense of satiety. Which is to say, after a meal that adheres to those dietary recommendations, do we feel full and satisfied, or are we still hungry? If the former, we’re apt to go along with the diet, but if we’re supposed to push our chairs back while our tummies are still asking for more, we’re apt to misbehave. A lot of it is subjective, of course, but experience tells us that some foods give rise to the sense of satiety while other foods make us want more. There are reasons why the appetizers tend to be savory, while deserts are sweet. Those tiny anchovies wrapped around capers raise the curtain on the feast to come and the butterscotch sundae brings it down. There’s some evidence that familiar foods induce the sense of satiety more quickly than novelties; the novelties – if we like them – cry out to us, “keep tasting!”
And it’s very clear that adherence is just about the most important consideration in evaluating the effectiveness of a diet. You can lead the horse to water, etc. A diet emphasizing a lot of soy-based meals has a very low glycemic load, and is also pretty cheap; whether many people will voluntarily stick with it is another matter. About five years ago there was a lawsuit in Illinois charging that the compulsory soy-based diet in Illinois prisons constituted cruel and unusual punishment; this diet was instituted in Illinois when that fellow Rod Blagojevitch was governor. Florida prison inmates have made similar claims. The soy prison diet exactly fits the third OED definition – a prescribed diet restricted in kind or limited in quantity, especially for penal reasons. Happily, for the majority of us not in Illinois or Florida prisons, diets are a matter of choice. But those factors apply nonetheless.
No condition or treatment area is more affected by these various factors than diabetes.
Diet and the current diabetes treatment landscape
Earlier in this piece, I noted that some diet experts had raised red flags in relation to milled whole grains, because they trigger the secretion of insulin which instructs the liver to store glucose as fat. This seems more than a bit contradictory in the context of diabetes, which (as the disease progresses) is characterized by insulin deficiency, so how could it be bad to trigger the release of insulin?
There is indeed something to it, however. The usual course of diabetes – we ‘re talking here about type 2 diabetes, usually abbreviated as T2DM – is that the individual’s pancreatic beta cells secrete more and more insulin in response to increasing glycemic load. The insulin receptors, which are in every cell in the body, get overloaded and are unable to respond to the insulin and convert the glucose to energy. The glucose cannot be converted to glycogen in the liver, which requires the action of insulin. Instead, it spills into the urinary tract. Lipids in the diet are stored as adipose tissue. The individual gains weight – a lot of weight. Eventually the whole mechanism of glucose metabolism crashes. And the individual, now diabetic, begins literally to starve. In the absence of a working insulin system, all that stored fat cannot easily be employed as energy. The prognosis for advanced untreated T2DM is not good.
Treatment for T2DM employs several strategies, which were discussed in previous Doc Gumshoe posts, 19 and 26 June 2014. (You can check all the old posts at http://www.stockgumshoe.com/author/mjorrin/.) But a common event in the course of treatment is that eventually, the oral antidiabetic agents, regardless of mechanism, stop working as effectively as they did initially, and patients need exogenous insulin.
When this happens, many patients gain weight. In fact, many patients whose diabetes is under good control, as assessed by their hemoglobin A1c levels, are overweight or obese. That’s because all it takes to keep HbA1c at a desirable level is enough insulin. Persons with diabetes monitor their direct blood glucose at fairly short intervals and base their insulin dosage on those immediate readings, not on the HbA1c reading, which provides an indication of what blood glucose levels have been over a period of several weeks. So it’s relatively easy for a person with diabetes to increase the insulin dose to compensate for what we might uncharitably call dietary excesses, and still keep their blood glucose at acceptable levels. But this can, and does, lead to considerable weight gain.
What kind of diet might prevent this? Perhaps not a prescribed diet, “as for penal reasons,” that doesn’t take into account factors like satiety and the likelihood of adherence, but a diet that might approximate a “customary course of living as to food,” tempered and moderate – a diet that most people could stick to for a long time. Persons with diabetes – along with persons desiring to shed some excess avoirdupois and persons wishing to avoid any of the ailments in the cardiovascular spectrum – i.e., nearly everybody … such persons are not prisoners, subsisting only on what’s in the tin dish shoved through the little opening in their cell doors. Such persons – that’s most of us – do not want to be Always Hungry and denied the pleasures of eating food that tastes good and makes us feel good.
Most nutritionists and, in fact, most of the clinical community, agree that what’s fundamentally wrong with the American diet is that way too much of what we eat is not really food, but food products, jazzed up with extra sugar, salt, transfats, and other stuff that’s no good for us. We’re too busy to buy real food and cook it, so we take short cuts, and those short cuts are a big part of the problem. There are certainly people out there calling attention to the situation – see Michael Pollan’s many books.
The diet gurus certainly recognize this, but with the best intentions, they prescribe diets that are hard to stick to. They need to put forward a provocative hypothesis to attract attention to their books or videos or whatever it is they’re using to promote their diet plan. Some of the ones who single out sugar as the villain of villains go so far as to warn against something as innocent as eating an apple, because an apple is nothing but a conduit for a lot of fructose. So much for “an apple a day keeps the doctor away.”
It’s easy to forget, when harkening to the preaching against sugar, that sugar – glucose – is the fuel that our bodies subsist on. Too much glycemic load certainly is a problem, for the reasons we’ve talked about. But let us not elevate tempered warnings into an absolute proscription. The simple-minded proclamations of some diets – “here’s the one fruit you should never never eat” – attract attention and maybe sell diet books, but they are not a pathway to a sustainable life plan.
Something that a lot of these diet gurus favor is dark chocolate, because is furnishes the right kind of fat – not transfats – and, we all hope, delivers the kind of metabolic benefits we’ve talked about here. David Ludwig says he eats low-sugar dark chocolate every day because of those benefits. But I suspect that daily dark chocolate is part of the provocative hypothesis – what was once forbidden is now mandatory.
However, the forbidden vs. mandatory axis is, in my opinion, a big part of what’s ineffective about prescribed diets. We want what’s forbidden, we shun what’s mandatory. A few of us may remember the famous New Yorker cartoon about broccoli: the kid, sitting at the dinner table, says “I say it’s spinach, and I say the hell with it.” If it becomes mandatory, there will be people saying the same thing about dark chocolate.
The diabetes treatment community, including the clinicians and the pharmaceutical companies, is keenly aware of the predicament posed by increasing rates of both obesity and diabetes, the increasing cardiovascular risks that these trends bring, and the discouraging results of diet plans as well as of many anti-obesity drugs. An encouraging development is that some diabetes agents now also have properties that keep the patient’s weight under control as well as his/her HbA1c. And the most recent and potentially best news is that a couple of newer agents have been demonstrated not only to control blood glucose and weight, but to confer significant cardiovascular benefits. The details of the studies confirming that bit of news won’t be made public until the American Diabetes Association has its annual meeting in June, at which time Doc Gumshoe will provide a full-scale review. The drugs in question are liraglutide (Victoza), from Novo-Nordisk, and empagliflozin (Jardiance), from Eli Lilly and Boehringer Ingleheim.
In the meantime, permit me to circle back to my point of departure: what we all need is a tempered and moderate course of living as to food. We should eat real food, experience pleasure at the dining table, and we should not have to push back our chairs feeling hungry.
There is absolutely no diet that will be effective if it denies you what you crave. Several years ago my niece who was suffering from depression was experiencing weight loss while on Paxil. I told my doctor and he humored me by prescribing Paxil which was not approved for that indication. I’ve been on it ever since. In my case it has completely eliminated my food (strong) and alcohol (less) cravings. As a result I have lost 45 lbs. and being a T2DM victim that was a Godsend. Walking the dogs 2 mi/daily has also helped. And finally my A1c in the low 7s while on Victoza. It also helped kill my appetite. Anecdotal but as a ChE, PE I must advise caution and recommend you consult with your health professional.
Cravings indicate something is wrong which needs correcting (not a drug). We can start with this radical concept: that you can’t feel satisfied when your body’s need for all nutrients isn’t met. Years ago Harvard Medical School released a sample diet based on nutrient-dense foods which provides all the daily recommended amounts of vitamins and minerals on just 1200 calories a day. So even eating that lightly while losing weight, you can be fully nourished.
http://www.health.harvard.edu/womens-health/getting-your-vitamins-and-minerals-through-diet
Very interesting, but I wouldn’t go that far and call meeting the DRI as “fully nourished”. The DRI is just the bare minimum “sufficient” dose to prevent overt diseases of deficiency, nevermind achieving optimal health (or therapeutic doses for treating non-pvert diseases). Look at how ridiculously low the RDI for D3 still is! Besides, that diet is woefully low in high-quality protein to offset sarcopenia and frailty. R.D.’s and nutritional academics rank among the most clueless about nutritional science. They just repeat the tired old institutional propaganda dogma as proscribed by the ADA (which is funded by the junk food companies, believe it or not) and the USDA. Nothing vanguard going on there.
Anyway, last time I looked at the issue of nutrients and diet, it would take about 27,000 calories to achieve ALL micro-nutrients:
“Analysis determined that each of the four popular diet plans failed to provide minimum RDI sufficiency for all 27 micronutrients analyzed. The four diet plans, on average, were found to be RDI sufficient in (11.75 ± 2.02; mean ± SEM) of the analyzed 27 micronutrients and contain (1748.25 ± 209.57) kcal. Further analysis of the four diets found that an average calorie intake of (27,575 ± 4660.72) would be required to achieve sufficiency in all 27 micronutrients. Six micronutrients (vitamin B7, vitamin D, vitamin E, chromium, iodine and molybdenum) were identified as consistently low or nonexistent in all four diet plans. These six micronutrients were removed from the sufficiency requirement and additional analysis of the four diets was conducted. It was determined that an average calorie content of (3,475 ± 543.81) would be required to reach 100% sufficiency in the remaining 21 micronutrients.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2905334/
Remember, “sufficiency” alone is worthless for anything other than just “getting by” in a suboptimal, low functioning state. So please don’t delude yourself or listen to ignorant crony capitalists like Dr. [Pr]Offit and his groupies. Supplementation is mandatory.
I agree with much in your first paragraph, but over many years arrived at a different solution than extensive supplementation. Our ancestors, before our soils became depleted and our foods perverted with refining and additives, were quite healthy and vigorous wherever/whenever they could survive childhood, infections, accidents, violence – and a lack of or insufficient variety of food. So trying to eat more as they did, whole foods only grown from healthy soils + some sea vegetables for trace minerals, has worked well for us. Replacing all grains and legumes with vegetables is a great idea too – vegetables are far more nutrient dense when you evaluate that by calorie rather than weight or volume. We usually take multivitamins as a little extra insurance but consider them far less important than where and how our food was grown or raised.
Patricia, you are right on target!! A perfect example of your “thesis” is grass-fed beef. That one food is so close to complete that it makes up (estimating here) about 60 to 70 percent of my diet. Grass-fed is to grain-fed (or finished) as a Van Gogh painting is to a pencil sketch.
I, by the way, am almost 72 (which still startles people who don’t know me), take no medications, BP 70/130, work hard every day, don’t take flu shots and don’t get sick even when everyone around me is hacking and sneezing.
Points well taken
These issues are especially critical when it comes to challenged immunity when recovering from illness or recovery from physical injury. I am forced to survive on a very restrictive vegan/neovegan regime due to extremely difficult dermal conditions which react to the nutrient-dense animal foods. (my MD says free-range eggs are about the best choice). I wound up chronically ill due to my work exposing me to little kid RSVs constantly, I stabilized once I added some eggs and fish back (now back to pure vegan due to what those foods do to my skin). This goes for injury recovery too, I remember how basketball star Bill Walton was an outspoken vegetarian until he had a nagging foot injury, he tried adding in salmon but when that didn’t work he wound up eating beef again.
I do an exotic array of “natural” supplements like sea veg/chlorella/beet root powder/ plus some pretty exotic root/bark extracts to get those critical minerals that I’m running the risk of shortage on due to no flesh. It does make a difference, also the “official” MD types are almost criminal in their disregard for the D3 issue, they’ve got everybody afraid of the sun now (natural light on the eyes does some hormonal-enzymatic reaction s too that no supplement will suffice for). I concluded from experience that everybody should do D3 in the winter, since I did it’s one of the factors that has kept me well through winters for the last 3 years.
My #1 Stock Pick for This Week Is… By Jeff Siegel | Tuesday, March 8, 2016
It all went down last Friday …
USDA Secretary Tom Vilsack made a comment that set off the alarms for investors in the agriculture space.
During a briefing with reporters, Vilsack voiced his support for the mandatory labeling of genetically-modified foods, after getting the nod that there could be enough votes in the Senate to get this kind of thing approved.
The theory is that if such a bill passes, it could mean big trouble for Big Ag, which relies heavily on genetically-modified foods, or what are often referred to as GMOs. Investors are also concerned that it could pose a huge threat for biotech firms like Monsanto (NYSE: MON), and Syngenta (NYSE: SYT).
As an investor who’s made an absolute fortune in the sustainable and organic foods space, I can tell you that I champion anything that could potentially add more value for organics and less value for the conventional toxic slop we call food today.
But despite the excitement in the treehugger camp of which I am a part, I can tell you, not as an environmentalist, but as an investor, that Big Ag and biotech investors have absolutely nothing to fear.
And here’s the most important part: If you get in now, on the ground floor, this emerging technology could turn every $1 you invest into $10… $25… even $50 or more… Click here now to seize this opportunity.
What Matters? Cheap and Easy
When it comes to food, I am obsessive.
I’m obsessive about where it comes from, who produces it, and how healthy it is.
Nearly everything I eat comes from local farms where I know the farmers.
My meat is raised in a sustainable manner where animals are treated with dignity and respect. They’re also fed what God intended them to eat — not toxic cocktails of GMO corn, growth hormones, and their own excrement.
Fruits and vegetables are grown organically, and anything “processed” is processed by me. I’m more than happy to bake my own bread, make my own sausages, and can my own vegetables. I even roast my own coffee beans, but that has more to do with me being a bit of a coffee snob.
In any event, the point is this …
Food is fuel. It’s medicine, it’s energy, it’s joy. So to put anything in my body that has been manipulated to the point where it’s no longer food, but rather various, re-formulated components of carbs, fats, and proteins is of no interest to me.
But here’s the rub …
I’m in the extreme minority, and folks like me don’t have enough of an impact on the global food system to even register as an accounting error.
Moreover, despite all the backlash against GMOs in the media, most people really don’t care.
Most people don’t even look at the ingredients labels on the things they buy.
Most people want food that is cheap and convenient. That’s it.
Sadly, most people don’t even use their kitchens anymore, other than to wash dishes and cook pre-made lasagnas in the microwave.
And here’s the inconvenient truth for folks who believe that mandatory GMO labeling is going to help people make healthier decisions when it comes to buying their food: It doesn’t matter.
The same people who are perfectly happy not knowing where their food comes from are not going to even notice a GMO label. And combined, these folks spend far more on their food than consumers of sustainably-produced and organic foods.
That doesn’t mean their value as consumers is insignificant. After all, the global organic market is currently valued at about $72 billion. That ain’t chump change, and it’s certainly been enough of a reason to invest in this space. Especially when you look at growth.
It’s not about the show, it’s about the GROW!
Between 2002 and 2011, organic food production increased by about 240%. Compare that to the 3% in the non-organic food market.
Yes, the conventional food market still controls the lion’s share of sustenance, but when it comes to investing, it’s not about how big the market already is, it’s about how big it can grow. And this is why I remain incredibly bullish on the organic food market.
I’m not saying every organic food play is going to make you rich. You still have to be picky, just like with anything. But there are still plenty of opportunities out there.
My favorite play in the space right now is Captiva Verde (CSE: VEG) (OTCBB: ARDWF).
This is actually one of the largest organic vegetable producers in the United States, providing a steady flow of organic vegetables to the nation’s largest supermarkets and food producers.
The company is well-funded and has a production capacity of 500,000 pounds per week. This is massive for this market.
Basically, Captiva is looking to become the largest producer of organic vegetables — mostly leafy greens — in the United States. And with demand so strong, and competition so limited, Captiva Verde is in a very sweet spot. It’s also a screaming bargain at current levels.
In addition to Captiva Verde, I’ve also covered a few private deals in the sustainable foods space. If you’re an accredited investor and would like to get in on some of these deals, you can do so by becoming a member of my private Green Chip Stocks service by clicking here.
To a new way of life, and a new generation of wealth…
Pump-and-dump anyone?
Interesting read as usual, but I seriously question the assertion that “…deserts are sweet.”
My understanding is that they are mostly hot and dry.
I live in a desert area, which can be pretty sweet for nine months of the year. And if that was the only typo in an article of this length, bravo.
> Something that a lot of these diet gurus favor is dark chocolate, because is
> furnishes the right kind of fat – not transfats – and, we all hope, delivers the kind of
> metabolic benefits we’ve talked about here. David Ludwig says he eats low-sugar dark
> chocolate every day because of those benefits. But I suspect that daily dark chocolate
> is part of the provocative hypothesis – what was once forbidden is now mandatory.
Uh no. Its the cocoa polyphenols. They’re cardiovascular protective. Not as good as pomegranate, but complementary.
Cholesterol and its transporters are poor correlates not primary causes. The core issue (of plaque) is endothelial dysfunction due to oxidized LDL vs nitric oxide (inverse relationship). The chemicals in fruits and vegetables that are excellent for maintaining a healthy cardiovascular system affect one or the other or both. It’s just that simple. Of course, there’s far more things than just the measly cardiovascular system to worry about in terms of optimal health.
Logically, a proper metabolic diet would have the carbohydrate intake at homeostasis, yes? Well, that’s at 30% of calories (athletes need more, of course). And, logically, another way to do a metabolic diet is to not stuff your piehole continuously for 16 hours a day and only in an 8-hour window. It’s just that simple.
Ultimately, its a CHOICE. You actively CHOOSE what is most important to you at the end of the day. Either be fat, sick and not quite dead or the opposite. Most choose the former because its the path of least resistance.
Our family’s cardiologist (Dr. Gundry, he wrote a book on diet) recommends one ounce of dark chocolate daily, 73% cocoa solids or higher. I’ve found that if I buy 85%, it’s bitter enough that I don’t want more than an ounce anyway! What is better though is a great hot chocolate I make with 2 TBSP cacao powder, 1/3 cup goat’s milk, 1 cup water, 1/2 tsp of vanilla, dash of salt, and sweetened with pure stevia powder.
Omg, sharing recipes on an investing site – obviously way past my bedtime and zoning out. G’night.
Patricia,
You are fortunate to have Dr. Gundry as your Cardio. My Cardio recommended the book and the diet to me. His book on “Diet Evolution” (mentioning it because I read it and recommend it) has turned my well-being around. The first 2 -3 weeks is the deal, tough, getting back to natural foods. Getting rid of unhealthy eating habits. No sugar at all. Well you got to read the book.
After 8 weeks on the diet my blood pressure is normal. Dropped 22lbs. in 4 months, without any special exercising other than walking. We have changed our grocery lists and our eating habits as a result. (Sugarless yogurt, almonds, walnuts, blueberries, strawberries just to name a few of the regular snacks or treats. At 75 & retired, I now work out in the Gym 4 to 5 days a week. Have plenty of energy. Continuing on to lose another 10 lbs.
More important to than investing is being healthy.
Thanks for your comments .
A few comments on the comments, and comments on the comments on the comments.
I reported on the benefits of dark chocolate in “Tidings, Mostly Glad,” on 18 December, 2013; you can find that post & others at http://www.stockgumshoe.com/author/mjorrin/. But I’m not too sure those benefits can be attributed strictly to the cocoa polyphenols and nothing else. I think one has to consider the total diet. When you eat A, do you therefore omit B from your diet? It’s thought that the worse health outcomes in people who consume large quantities of diet soda may be due to their eating large quantities of junk food. And back in the 1970s there was an epidemic of kwashiorkor (severe protein deficiency) in middle class teenagers in Denver, which was attributed to their subsisting largely on soda pop. It’s the “what do you eat instead” phenomenon. People avoid the bugaboos and compensate with food & drink that is often worse.
I would like to blame the “deserts” typo on autocorrect. Or else on my wife, who proofread the piece. Rats!
But I firmly and deeply believe that what’s essential to health is the simple desire to live and enjoy life. I am getting on in years (82) and would like to sing the Monteverdi 1610 Vespers again before long, as well as the B Minor Mass. I look forward to every meal with a lively appetite. And I ain’t fat! Best to all, Michael
Many more good years to you Michael! I can’t scientifically critique the various studies on the benefits of chocolate, but can share my own experience with it. Typical sugary chocolate candy, desserts: bad! Made me feel lousy, many negative effects. But homemade cacao treats, sweetened with stevia and sometimes a little honey: good! Never have had the slightest problem. In fact, one or two mugs of the hot chocolate I described in a post above is often my only breakfast and keeps me satisfied and going often well past noon. This still mystifies me a bit. I came across a reference recently indicating that the early Spaniards noticed it too – that they could march much longer after having cacao. I don’t think it’s just the stimulants in it, because the energy it gives me is of the calm, natural kind, nothing like a nervous caffeine rush. Cacao is a whole, balanced food in its natural form and it’s wonderful to enjoy it guilt-free.
Thanks for your articles and for tolerating those of us (OK, mainly me) who go overboard with our number of comments. You sometimes write on subjects that are close to my (healthy) heart.
Hi Patricia:
Thank you for passing on your experience with cacao to start the day. I am going to give it a try as soon as I can get to No Frills on my mountain bike for the goat’s milk. (One of my younger brothers had goats when he lived back in the hills years ago and gave me a glass of the stuff. I still remember the incredible creamy texture and rich flavour.) I’m going to need all the energy I can get for the impending gardening season.
Apologies to “Doc” Jorrin for my sarcasm. I have said before that I appreciate the exceptional writing standards and readability of Stockgumshoe.com, but, as Oscar Wilde once said: “I can resist anything but temptation”.
Regards to all from here in late-winter Canada.
Doc Gumshoe,
I just happen to be a retired doctor , ( and RN before that), and I must say, I always enjoy your articles and their reasonable approach .” Moderation in all things”, as Aristotle put it. That is the primary reason I am going to join up with Stock Gumshoe today , along with TJ’s healthy cynicism and honesty. Thank you all- for the moments of sanity .. you have earned my tithe !
Welcome to the Gummune ET 🙂 Best2YouAlwayz-Ben
I am struggling with moderation but I find the weight just keeps creeping on. I prepare almost all my family’s meals from scratch, always including fruits and veggies. We limit chips and similar snacks and most desserts are home made. But it is so hard, especially with kids and a family tendency to obesity! Everywhere you go there is food available or the kids are given a snack time. I often feel very discouraged.
Great article — thanks. When may we expect the follow-up mentioned in the second-to-last paragraph. (Yeah, I could’ve said penultimate, but I ain’t that pedantic.)
More about diabetes – in the hopper!