 Of Needles, Haystacks, and the Needle-in-a-Haystack Cancer Diagnostics Nanocap That May Belong in Your Portfolio
Of Needles, Haystacks, and the Needle-in-a-Haystack Cancer Diagnostics Nanocap That May Belong in Your Portfolio[Ed. Note: Here is the latest from Dr. KSS, who writes about health, medicine and biotech stocks for the Irregulars. He has agreed to our trading restrictions, and his words and ideas are his own.]
Dedicated to Cynthia Chew Choon Hoon (1959-2013). In pace requiescat.
Imagine a day down the hallway of the future. You’re a happy Gumshoe Irregular, you’ve just turned 65, and last week, you had a routine check-up with your doctor. You feel great and are looking forward to a contented, ebullient retirement. It’s early evening. You and your wife are having gin-and-tonics on the veranda, watching the sunset. The lime in your drink is tart, zesty, and life is good.
But the phone rings. Your wife answers, ignoring your importunings that she ignore it. She beckons you. It’s your doctor, and he wants to speak with you. Can’t be good.
The doctor is still in his office going over labs and test results, and decided to call you rather than sending a letter. Last week, he drew a PSA and also examined your prostate. It seemed fine. But it’s your PSA that concerns him. It is now 4.5, not screamingly high, but up from last year’s level of 4. He wants you to come in again.
You imagine a device being shoved into your rectal vault, from which lots of needles will suddenly extrude and plant themselves painfully deep into your prostate gland, translocating germs from your rectum into it, causing bleeding for days on end…and you begin feeling dizzy. Your ears begin to ring, you break out into a cold sweat. Your worst fears are coming true, you begin seeing spots, and slide onto the floor. Little birds fly around your head.
“Hon?! Are you OK?,” your wife shouts.
“Hello……sir? Are you still there?” the doctor is shouting into the phone.
Your wife grabs the phone. “Doctor, my husband just fainted!”
“Is he OK?”
“Just dizzy and sweaty. He’s coming around.”
“I must have scared him. I told him his PSA is high.”
“Yeah, he mumbled something about prostate biopsies? I think that put the fear of God into him.”
“Prostate biopsies? I didn’t say anything about that.”
“Isn’t that what you are planning doctor?,” your wife asks.
“Well, no, not at all. I just wanted him to come back so we could draw blood, you know, to look for any prostate cancer cells. Prostate biopsies? No, we don’t do those anymore.”
Medical science fiction? Probably not. The lab test in question, looking at blood to find circulating tumor cells, is now making its first forays into prime-time, though as of yet it is to assess response to cancer treatment rather than in place of tumor biopsies. But that is likely to change, and in fact one tiny biotechnology company seems uniquely poised to benefit from this new science and this emerging “hot”new diagnostic trend.
Do you remember this scene from The Silence of the Lambs? Have a look. Clarice Starling is wrestling with the identity of a killer, and Hannibal Lecter, trying to act as her mentor, encourages her to think like Marcus Aurelius and mull the essence, the nature, of the killer.
Cancer is a killer. But what is cancer, in its essence? What is the nature of cancer? What distinguishes cancer from all other illnesses? What does cancer do that no other disease does? There’s an old word I love, quiddity, sometimes defined as that which answers the question, quid est? What is the quiddity of cancer?
Cancer spreads. It metastasizes. That is the most scary aspect of its nature. Cancer is like a flea that bounds from place to place in the body, and takes up residence easily at sites remote from where it started. Yes, cancer can extend locally, but it loves to end up at distant sites without leaving any crumbs for how it got there. How does cancer get to those places? Some will answer via the lymphatic system….that cancer goes to lymph nodes and from their more broadly into the body. But there is a better answer.
The fact is, cancer cells get into your bloodstream, and course around as if they were river rafting. And this idea is not a new concept. When they reach a rivulet, a capillary, a tight spot from which they can flow no further, they lodge. They take root there. Most of these attempts at colonizing, at metastasizing, provoke immune reactions that are deadly to the tumor cells.
Armand Trousseau (1801-1867): A Gregarious Master Clinician
Nineteenth-century France gave the world many fine physicians, including Dupuytren, Duroziez, and the astonishing Rene Laennec. But none were more remarkable than Armand Trousseau, an affable Paris internist.
On 27 June 1867, Trousseau died…to the shock of friends, patients, colleagues, seemingly to the surprise of everybody but one person: Armand Trousseau. He was 65. In January of that year, he had noticed something amiss in his left upper arm. One imagines him at a wash basin with a straight razor shaving around his bushy sideburns, and feeling a pang. He noticed a painful, tender, hot mass in his arm, a blood clot. The next day it had subsided and the mass and pain were gone. He knew what was coming, and knew he had at most 6 months.

The eminently likable Armand Trousseau, MD. Il a découvert et puis il l’a tué
Trousseau had many fine accomplishments—better treatments for COPD, malaria, pleuritis, goiter, yellow fever; he performed the first tracheotomy in France—and was also famously known as a patient advocate and a person who became so absorbed in listening to and studying patients at their bedside that he lost track of time. In Irving Stone’s fine historical novel about Sigmund Freud, The Passions of the Mind, he depicts a scene in which, at a teaching hospital bedside, the great Charcot extols the virtues of “see-ing,” of really opening one’s senses and studying patients, of even ignoring one’s education somewhat and letting bedside findings, primary observation, guide you in formulating disease and its treatment. Paracelsus admonished physicians always to let patients be their true textbook, that observing patients never deceives. Trousseau paid attention to patients, and little escaped his notice.
 In Choruses From “The Rock,” T.S. Eliot asks, “Where is the wisdom we have lost in knowledge?” Trousseau would have sympathized with this, because regardless of his learning, regardless of what he had read, he always noticed the details of what he observed with every patient. “Get the patient well!” was what Trousseau always told medical students, and it was with patient centeredness in mind that he noticed a process no one else had: the phenomenon of migratory thrombophlebitis, later known as Trousseau syndrome. Trousseau noticed that certain people would have acute venous thrombosis with local inflammation in a limb, with disappearance of the process one or two days later, and that patients always died within 6 months of a visceral cancer, malignancy somewhere in the abdomen. He hypothesized that cancer somehow distorted the clotting system, favoring thrombosis (he was correct…except that rarely prostate cancer favors a bleeding tendency). Later observers also noticed that lung cancer causes Trousseau syndrome. And in fact, pace Trousseau, patients who have an unexplained episode of deep vein thrombosis need underlying cancer excluded. (Trivia question for medical readers: what is the Trousseau sign?)
In Choruses From “The Rock,” T.S. Eliot asks, “Where is the wisdom we have lost in knowledge?” Trousseau would have sympathized with this, because regardless of his learning, regardless of what he had read, he always noticed the details of what he observed with every patient. “Get the patient well!” was what Trousseau always told medical students, and it was with patient centeredness in mind that he noticed a process no one else had: the phenomenon of migratory thrombophlebitis, later known as Trousseau syndrome. Trousseau noticed that certain people would have acute venous thrombosis with local inflammation in a limb, with disappearance of the process one or two days later, and that patients always died within 6 months of a visceral cancer, malignancy somewhere in the abdomen. He hypothesized that cancer somehow distorted the clotting system, favoring thrombosis (he was correct…except that rarely prostate cancer favors a bleeding tendency). Later observers also noticed that lung cancer causes Trousseau syndrome. And in fact, pace Trousseau, patients who have an unexplained episode of deep vein thrombosis need underlying cancer excluded. (Trivia question for medical readers: what is the Trousseau sign?)
Trousseau was among the earliest popularizers of bedside, patient-based teaching. When he had interesting or complex patients, he would summon students and trainees for long, impromptu sessions in which they gathered around the patient. Trousseau would hold forth, and recite the patient’s history with a novelistic richness, a raconteur’s vim and vigor. This often charmed patients, that he had gone to such pains to know their histories in depth. And he often amazed patients with insights about their lives, their motivations, their relationships….things they recognized as true, but had not recognized before. Many physicians who love teaching at the bedside—and I am one—love it for one reason: the teacher gets to midwife the forging of new neural links, new understanding….gets to be present at the birth of knowledge. Students are asked what they see, and how that may relate to something else they’ve seen. With the right Socratic bent, five minutes at the bedside can teach a student vastly more than six weeks at the books can, but also tends to do so with a suddenness that thrills. The ice floes of book understanding break up, and the white water of real comprehension flows. The student gets a look on his or her face suggesting that serotonin, dopamine, glutamine and norepinephrine are flooding their synapses in unison: they get it now, they never got it before, and they will never forget it. You don’t do this so you can take credit for it, and in fact you do not care if the student even remembers that it was you who helped them learn. You just want to be there for the epiphanies, the fleeting moments when a student’s eyes, brow, and lips convey that they just underwent a cognitive firestorm, and that several brain neurons that had never met are now hopelessly, inextricably intertwined.
At the height of his reputation, Trousseau delivered a fine lecture in Paris on the phenomenon of migratory thrombophlebitis, which he called phlegmasia alba dolens:
“I have long been struck with the frequency with which cancerous patients are affected with painful edema in the superior or inferior extremities, whether or not either was the seat of cancer. This frequent concurrence of phlegmasia alba dolens with an appreciable cancerous tumor led me to the inquiry of whether a relationship of cause and effect did not exist between the two, and whether the phlegmasia was not the consequence of the cancerous cachexia.” (translated from the French)
An autopsy on Trousseau showed he had advanced gastric cancer. The jovial, inspiring doctor was dead. He is still quoted in medical training programs all over this planet for his shrewdest utterance: “utiliser de nouveaux médicaments rapidement, alors qu’ils travaillent encore” (“Use new medicines quickly, while they still work.”) Even before the days of Big Pharma and vaunted claims for new medicines, Trousseau was aware of the meta-placebo effect, placebo by proxy: that sometimes newly-released medicines work, or seem to, simply because physicians have great faith in them.
Theodor Billroth, the famed Prussian-Austrian surgeon who was a contemporary of Trousseau, would go on to identify pancreas cancer cells rarely found embedded with clumps of platelets in the capillaries of pancreas cancer patients. Billroth never published this, but noted it in his personal papers. One wonders if Billroth, who advanced the art of visceral surgery considerably, could have saved Trousseau. Billroth was a personal friend of Johannes Brahms, an excellent musician, and often proofread and helped Brahms rehearse his pieces as he was writing them. Brahms would go on to die of a mysterious jaundicing illness that baffled Billroth, and about which I have long meant to publish a theory.
Theodor Billroth (1829-1894). Before there were Billroth-I and Billroth-II procedures, there was Billroth the man. He performed the first successful gastrectomy for gastric cancer in 1881.
Two years later, in 1869, Thomas R. Ashworth, a Melbourne physician, would publish the literature’s first description of circulating tumor cells in Australian Medical Journal. Ashworth had a patient who died of advanced cancer, and at autopsy found occasional cells in the patient’s blood identical to those in the cancer.
Black swans, hens’ teeth, four-leaf clovers…. and black cats in coal cellars
It’s not clear that Ashworth knew of Trousseau syndrome, or would have appreciated what would later be recognized (vide infra), which is that tumor cells trigger platelet aggregation and that this is responsible for what Trousseau observed. But like many Australians, he was clever: tumors did not metastasize via a Star Trek transporter (or choose a 19th century analogy). Best to go looking for individual tumor cells, then, loose and afoot in the system. He found them….cells in the blood identical to cells in the tumor. Looking for them was like looking for a black cat in a coal cellar. One of the ironies of Ashworth’s description of the patient and the cells is that no one has ever known for sure what kind of cancer the patient had. Ashworth described subcutaneous nodular cancer, and many feel he may have been reporting a case of soft-tissue sarcoma.

White peacocks, red bananas, insanely big crabs. Australia has always given the world rare things, like the discovery of circulating tumor cells. One thinks of black swans as rare, until you cross the Hobart, Tasmania, bridge over a waterway inhabited by them!
When cells grow in organs, they do so in an orderly, non-aggressive, well-behaved way, not violating boundaries, displaying inhibition at contact with neighboring cells. Cancer cells do not scheme badness, do not plot ways to subvert the system. As we are all of us evolved, so cancer represents certain elemental steps that go on in evolution: DNA occasionally rolls the dice, rearranges itself. Occasionally certain rules get subverted. Humans fancy the ideas of immortality like the gods have. And so it, seems, maybe do cells. They stumble upon ways to live forever, and to propagate themselves by growing aggressively and even escaping their confines, becoming flotsam and jetsam that catch blood currents to other locales. It’s not that the cells go rogue and plan to cause trouble. But gene rearrangements and mutations confer properties on cells that harm the organism, and when enough errant properties, including the abilities to invade, metastasize, repel the immune system and resist intrinsic mechanisms of apoptosis come together, the result is cancer and it kills. Humans long for, dream of, immortality. Is there a reason our cells should not do the same? (And is it possible that our craving for immortality is hubristic because it is harmful to some greater system (Jung called it the Collective Unconscious), just as cancer harms us, that we comprise but know only through-glass-darkly?)
If you have cancer, how likely are you to have circulating tumor cells? No one knows. In fact, this is a question today’s featured company may help medicine answer. Certainly the more advanced, the larger, the more inclined to metastatic spread a tumor is, the likelier it is to have breakaway stray cells found in your blood. The number of cells in a cancer is proportionate to the volume of a tumor. From geometry, we know that the volume of a sphere rises as a function of the radius to the third power. Which means that when a tumor doubles its diameter, it has 8 times as many cells as it did at its former size. So the number of circulating tumor cells should be strongly linked to tumor size, and in fact a test for circulating tumor cells as a global screening test for any kind of cancer as part of a wellness check is unlikely to happen. We will always need to continue to pay attention to organs—-breast, prostate, colon, the lungs of smokers, the skin of the Celtic and the immunosuppressed—-known to be trouble spots.
Here are some number to give you a sense of scale for the prevalence of circulating tumor cells. One liter has one million microliters, or 1000 cubic centimeters. One cubic centimeter is one milliliter. Blood has roughly one million red blood cells per microliter. Blood may have about 1000 white blood cells per microliter. But in a cancer patient, blood may have only 100 to 1000 circulating tumor cells per liter; that’s one circulating tumor cell for every one to 10 cc’s of blood.
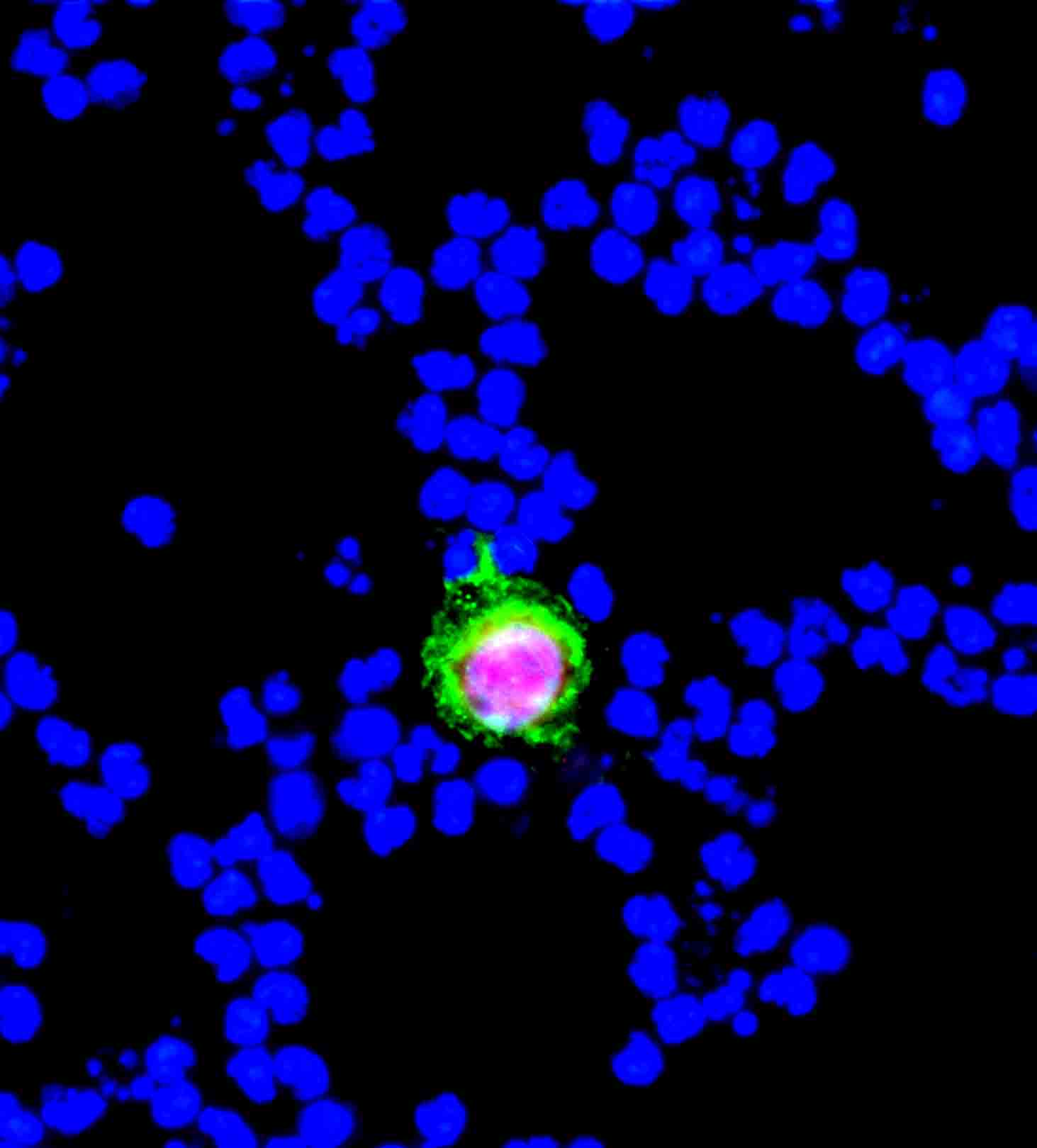
Technology makes it easy to spot this circulating prostate cancer cell in blood. T.R. Ashworth had no technology…it was Australia 1869 for him. (From Genelux.com)
Huahsi Night Market (華西街夜市)
In 1991, I packed and departed for Taipei. Circulating tumor cells have long fascinated me, and I was intrigued by data that circulating tumor cells often break loose only to provoke platelet aggregation around them. The tumor platelet clump may form a bigger vessel for a voyage, and once it lights or lodges at some point, the platelets release molecules that act as growth factors, fertilizer to jazz up tumor growth. I wanted to study this further, and in fact had heard of a viper unique to Taiwan with a venom component that seemed able to halt the process.
Taipei has many fine night markets, but the one at Huashi is notorious. Handlers taunt and irritate cobras while you watch, take extraordinary risks with them, and then kill them, slick them open with a knives or scissors, and empty the snake’s bile and blood into a glass of strong liquor (ask Irregular Eddy to tell you about the vaunted properties of this cocktail). I did not handle any snakes in Taiwan, but we relied on handlers like these to provide the venom for our studies.

Huashi Night Market, Taipei, Taiwan. “Snake Alley.”
We were able to demonstrate that when we grew human breast, prostate or colon cancer cells in culture, and then made a suspension of intact tumor cells, those tumor cells would immediately provoke full aggregation, or clumping together, of platelets. When blood clots, there are two waves of it: primary hemostasis, in which a platelet plug forms at a site of injury, and then secondary hemostasis, in which (as per the article on Regado) insoluble fibrin is formed from soluble proteins in blood. Normal cells do not cause platelets to aggregate. Most tumor cells do, and with considerably potency. What’s more, the avidness with which tumor cells provokes platelets to aggregate, we showed, is proportional to how much metastatic potential they have.
What Trousseau was observing, in fact, was circulating tumor cells (some, but not all) causing tumor-cell-induced platelet aggregation. These clumps would lodge, set off an inflammatory process, but also because not enough molecular stimuli were present to provoke a full and thick clot, would probably set into motion clot-dissolving machinery (fibrinolysis), and the tumor cell/platelet clump break up after 1-2 days.
Tumor cells appear to express uncommonly high levels of tissue factor. As in the Regado article, this is a cofactor for factor VII, and when these two merge, they afford thrombin. Although collagen, epinephrine, ADP and thromboxane are platelet agonists, thrombin is the physiologic platelet agonist, and triggers platelet clumping even when present at concentrations too low to cause fibrin clot formation.
Cancer: Metaphysics, Semiotics, and Metaphors
In the late 90’s, I found myself late one summer in a situation I am sure other readers have. I was exhausted from working hard. I had a vacation week coming, but somehow had planned nothing. But I really needed to do something fun and diversionary. At the very last moment, I booked bargain passage to Budapest, seemingly the last quarter of Europe I’d not seen. I had literally packed for it by throwing things into a knapsack while a cabdriver was outside angrily blowing his horn. I was in a state of physical depletion when I left, so much so that upon renting a car in Budapest, I pulled over in a public park, stretched out on a table, and dozed off and began dreaming. I woke up feeling good, and drove off in earnest toward Slovakia, into a park near the magnificent Aggtelek Cave system, and found a wooden cabin. In chill mountain air, I turned on an incandescent lamp at the head of the bed, reached into the knapsack and fished out two books I had long meant to read: Susan Sontag’s Illness as Metaphor and AIDS and Its Metaphors. I didn’t doze off again til dawn.
Sontag wrote the first of these books in 1978, when she was being treated for breast cancer. She deeply explored the metaphorical meaning then attached to cancer, which at the time was that somehow cancer patients had brought the illness upon themselves as a consequence of pent-up, anxious, fretting, repressed personalities. Psychiatrists attached themselves to this belief system, advocating psychotherapy to disabuse patients of the mindset, the hang-ups said to have led to their cancer. All one needs to do is spend some time at a cancer center (I formerly was on the faculty of MD Anderson Cancer Center) and you realize: this is an illness that strikes anybody, everybody, and there but for the grace of…
We know now this was nonsense, that cancer is a set of errant molecular events with no more moral or mental dimension than a head cold. You would not see a priest for pneumonia, so why see a psychiatrist for cancer? And yet even in our time there are those that still attach metaphors to cancer, often metaphors that stand to advance, to be in service of, other belief systems. I have had deeply religious patients tell me that ministers are trying to draw them deeper into the religious fold, that they’ve been told that unconfessed sin is manifesting itself as their cancer. Those same patients have been propositioned by the execrable practitioners of vitamins, herbs and the alternative, with claims that the illness owes to a lack of naturalness, to vitamin deficiencies, to quaint “imbalances” and that they know solutions (solutions from which these advocates always stand to profit). Mantra recitations do not cure mutations.
As Sontag identifies, other metaphors, still deeply trenchant, have attached themselves to tuberculosis and to HIV. I worry there may be readers here who have cancer, or who will face a diagnosis of it, who view this as the final horrifying intimation of mortality, that a cancer diagnosis is evidence of a body giving up, of a system whose machinery has gone irrevocably haywire, and that things will never be the same. Don’t. In fact, every day you are alive, somewhere in your body, you have cells undergoing transformation to cancer, ones that are conquered by various mechanisms (immune kill, apoptosis). That one of these improbable events serializes and compounds itself….these are, chances have it, things that will befall all of us given world and time enough. Anticipate. Expect. Screen. Pay attention. If and when it appears, play to win and take no prisoners.
In the threads we have discussed personalized medicine, the idea that your genes define you and provide all one needs to know about you. I am a dissident of this view: not all genes are expressed, and even for those that are expressed, we are only now in our earliest stages of understanding what turns expression of those genes on and off. This is the field of epigenetics. What is a four-dimensional printer? It is a three-dimensional printer that in hidden ways confers on the three-dimensional product attributes that allow the printed product to take on structural attributes not strictly reckoned by its three-dimensional printing. In a way, the genome is a 4-D printer: it makes a stew of proteins and RNA, and somehow that stew rises above the DNA sequence and controls it, decides what will be expressed, how and when. We are several Nobels away from a full sense of the science of epigenetics. For eons, people have argued genes versus environment, nature versus nurture. But the truth is it is neither, and both: the products of the genome, in the context of environment (temperature, nutrients, chemicals, and maybe softer constraints, such as social issues), have an amazing way of regulating the genes and how they genes behave. It is neither nature nor nurture. It is both nature and nurture, acting not as independent forces but in combined ways we don’t fully understand. It is what happens at the mysterious intersection of genes and environment that defines us. For many psychiatric illnesses, we now have a sense that it may not be a gene, and may not be a traumatic experience, but may be that the traumatic experience has permanently affected the expression of a gene. Which means that neither psychotherapy nor traditional psychotropes may help it.

In the comedy Trading Places, the fates of an investment banker and a street criminal are swapped to settle a nature versus nurture bet between two rich addle-brained aging brothers. Both lose out, in poetically just ways.
When a lump is found in a breast, when a PSA is sky-high (not 5 but, say, 50), when masses are found at colonoscopy, biopsies are done, tissue is obtained. Why?
That may seem a dumb question. The old answer was: to establish or exclude the presence of cancer. That age may be passing, however. Multi-detector CT imaging, now four-dimensional (the fourth dimension being temperature), already provides so much data corroborative of cancer that biopsy may be superfluous. A former colleague of mine, a radiologist, has become literally a chemist: he is a very bright man, and is actively developing a novel new set of radiologic imaging agents that have such unique ways of binding to tumors (and binding only to those tumors) that they may lead to imaging techniques that totally remainder the need for biopsy. For years I have had recurring arguments with oncologists over one situation: that of the cirrhosis patient with a 5 per cent per year risk of developing hepatocellular carcinoma. The patient’s alfa-fetoprotein is now 1000 (and his testicles are normal), and there is a mass that enhances in the arterial phase of a contrast-enhanced CT scan. If a biopsy of such a mass showed no cancer, would that mean anything? Would you trust that negative biopsy? I say “of course not!” You only do a test when the result will affect patient treatment. And I say, in fact, that we subject that patient to danger by sticking a needle into a safely encapsulated, walled off tumor, spewing its cells everywhere.
There is some necessity of biopsy, of course. As a medical student, I was peripherally involved in the case of a man who had an large opacified mass in his right lung. The mass could not be reached bronchoscopically, but he was bronchoscoped anyway, to look for other evidence of cancer. Washings suggested cancer cells though no cancer was seen. The patient went to the operating room, and his right lung was removed. When that lung was breadloafed up later by a pathologist, the mass proved to be a giant fungus ball, and there was no cancer. The cancer had been in the patient’s left lung, not yet apparent on CT.
A more modern reason for doing a biopsy is the personalized medicine thing: not to make a diagnosis of cancer, but to extract DNA from the cancer, and find what genes, what markers, are present, so as to guide chemotherapy. But in one of the threads, I argued that this has its problems too, and provided references. Tumors are famously heterogeneous, and a needle may have been stuck into a part of the tumor where cells simply lack the markers that will most define the overall cancer’s response to chemotherapy.
But some data, new and very recent, suggest that if one looks at circulating tumor cells, one may get the best reveal. It’s like not looking for Hollywood stars on the internet, but going straight for the Walk of Fame. The “baddest,” the most ill-behaved, most metastatic, most aggressive of the cells in a tumor may be those that pop off into the circulation.
Which is where an interesting new company comes in…
Biocept (BIOC) is a tiny San Diego company ($23 million market cap) that went public on 5 February 2014 with 4.5 million shares. I have taken a position in this company, as risky as it admittedly is, because I regard its circulating tumor cell detection methodology as best of breed.
Biocept has a proprietary method for detecting rare circulating tumor cells using a combination of multiple monoclonal antibodies (with a final avidin-biotin binding step) and complex microfluidics. It does have competition. Janssen Diagnostics (a unit of Johnson and Johnson) has a competing methodology, its so-called CellSearch machine, which several large national reference labs own. An excellent recent study, done admittedly by Biocept, compares Biocept’s method head to head with that of Janssen for detecting breast cancer cells. I have read the full text of this article, and am persuaded that Biocept’s method is superior. It claims an overall detection rate of 89 percent, versus 69 percent for Cellsearch, but for certain specific types of hard-to-find cells, Biocept’s is three times likelier to pick them up. And a success for Biocept in this arena is likely to make the stock catch fire, while broader implementation of CellSearch machines is unlikely to budge JNJ share price. I am long BIOC and have no position in JNJ.
Where Biocept’s method really outshines Janssen’s however, is as regards characterizing the cells it detects. FISH analysis is fluorescent in situ hybridization. Since a strand of RNA or DNA only binds to a complementary strand, it is possible to “probe” a cell isolated by Biocept’s method using diagnostic nucleic acid pieces, look for the presence of oncogenes.
HER2 is an important cancer marker found in about 20 per cent of breast cancer biopsies. The presence of HER2 strongly influences choice of chemotherapy. Women with HER2-positive tumors need therapy with Herceptin, a monoclonal antibody. Biocept published a fascinating study in 2013. Tumors are heterogeneous, and Biocept has evidence that a sizable number of women with HER2-negative tumors by biopsy actually have HER2-positive cells disseminated from the tumor in circulation. This is revolutionary, as those women require and will live longer with Herceptin-based regimens, even though their old-fashioned tumor biopsies said Herceptin would be neither helpful nor necessary. And there is an inherent logic that these cells would be the ones that make in into circulation: HER2 confers aggressiveness and metastatic potential on breast tumors. HER2 is a receptor tyrosine kinase related to the epidermal growth factor receptor.
Biocept is actively developing validated tests for lung cancer, prostate cancer, melanoma, and GI malignancies. Biocept’s methodology is sweetened considerably by the fact that in many aggressive tumors, in the rare cases that circulating tumor cells cannot be found, circulating tumor DNA can be found. Its methodology can detect that, something CellSearch’s cannot do. Biocept’s CEE (for cell enrichment and extraction) can sniff out tumor DNA in a sample, and probe that for tumor markers.
These are the kinds of tumors Biocept’s method can help diagnose and guide therapy for, arranged in order of deadliness:
| Cancer type | Deaths/Year | New Cases/Year | People living with diagnosis |
| Lung | 159,480 | 228,190 | 399,431 |
| Colorectal | 50,830 | 142,820 | 1,154,481 |
| Breast | 39,620 | 232,340 | 2,829,041 |
| Prostate | 29,720 | 238,590 | 2,617,682 |
| Melanoma | 9,480 | 76,690 | 921,780 |
These are statistics about Americans.
Are there risks to being in Biocept? Certainly there are, and this investment is not right for the intensely risk-averse or for a sizable part of your portfolio. My personal view is that its growth prospects are enormous, even extraordinary, even though I rarely invest in diagnostics plays. The technique is new, the methodology the company owns is definitive, and Janssen seems not intent to compete. I feel diagnostic testing with this system will be standard of care within 5 years. But herein lie risks. One is that the FDA has not approved these tests, simply because the field is too new. Approval…for what? For making an initial diagnosis? In lieu of biopsy? As a means of monitoring response to chemotherapy? The method is too new for the company even to know for what it should seek approval from the FDA. The company has many collaborative investigative arrangements with many American institutions, including MD Anderson. Meanwhile, I have spoken with the company and it is quite clear that insurers are reimbursing it for these tests, done at its facility in San Diego, because such testing is preferable to and cheaper than repeat biopsy to guide therapy. So many global institutions now have home-grown studies of ways to pick up circulating tumor cells and looking into their relevance, there is definitely the possibility that some other biotech could yet find a better method. Having read about the methods, however, I am inclined to doubt the would-be competition.
You probably have many questions.
(1) Will Biocept’s method ever totally replace tumor biopsy? That’s too early to call, but it seems probable it will, at least in some cases. The sensitivity of the method is quite high. The company will have to do studies to document the presence of circulating tumor cells in a variety of cancers and get a better sense of how advanced the cancer has to be before it can be detected in blood.
A close friend in Asia recently lost a non-smoking sister, with young children, to lung cancer. Although radiographic evidence screamed that she had cancer (she had a routine chest x-ray, which led to a CT), fear took over, and denial intervened. An unscrupulous traditional medicine practitioner fanned her denial, and promised a cure with Chinese herbs. It could not be cancer, she said. I am healthy and I have never smoked, and besides if it is, I have these herbs. This was a smart woman, a documentary producer, in one of the world’s great cities. There was also the grim reality that to prove it was cancer would involve hospitalization and a grisly procedure, called transthoracic needle aspiration, that would in all likelihood collapse her lung and would in all certainty be agonizing. Except for giving birth, she had never been hospitalized. She was warned by me that she had, at best, 18 months to live if she refused treatment, but that resection would likely cure her. She refused. Her brilliant unconscious was not subject to the rules of transparency and accountability that her brilliant consciousness used, and it slipped off into the dark; it did its calculus and demanded denial as a plan of action. She could not cope with the dissonant truth of cancer. 17 months later, she became quite confused…from brain metastases. One month later she died. Her children are still at home, and motherless. And yet had Biocept’s system been available, a mere blood draw could have provided proof positive of lung cancer, and guided therapy (surgery, drugs, radiation, or what combination). Had Biocept’s method been available, she might now be alive: the data would have convinced her she had cancer that was serious and invasive.
A fascinating just-published study in Nature Medicine, unrelated to Biocept’s efforts, raises the possibility that methods to catch circulating tumor cells are so good now that such cells might be propagated outside the body, in culture or in mice, and then characterized, DNA-assessed, in order to predict response to various interventions. The cells could isolated from a tube of your blood, placed in a mouse, allowed to grow, then harvested and their DNA deep-sequenced.
(2) Will Biocept’s method ever become a screening test for cancer? Many medical professionals reading this may recall a now-nearly-forgotten New England Journal of Medicine paper from when I was in medical school that showed a difference in nuclear magnetic resonance spectoscopy signal between blood of people with and without cancer. The test would give no clue as to type of cancer, of course, and neither could it necessarily be reliable for picking up early stage disease. We will continue to need to screen high risk organs, such as breast, prostate, and colon. Japanese people in Japan will still need screening upper endoscopies at age 40 because of the high risk of gastric cancer in that setting.
Will it ever become a routine blood test to look for cancer? I suspect it will not be priced to make that affordable, and not covered by payers, but if a patient is having other symptoms or labs suggestive of undiagnosed malignancy, it may be considered. Certainly given the breadth and specificity of the testing antibodies Biocept has, it is reasonable to predict that from the blood test, it could narrow down what organ is involved in the cancer.
Again comes the question, however, of whether it will replace biopsy. If the test picked up a cell likely from the pancreas, and the patient has a radiographic pancreas mass, at present oncologists would refuse to treat that patient without tissue from the pancreas lesion showing cancer. With time, with proof of Biocept’s method, with oncology getting farther down the learning curve of this method, however, that may change, especially at academic centers.
(3) If I have cancer, have had a biopsy, and am receiving treatment, does Biocept’s method have anything to offer me? It very much does. Tumor behavior, tumor oncogene expression can change with time, on the basis of what drugs have been given. Those drugs may kill off sensitive tumor parts, and select for resistant cells. Biocept allows determination of this without another biopsy.
The time may come, depending upon price, when circulating tumor cell burden is used as a way to follow response to chemotherapy, much as repeat CT to measure lesion size now is. This fascinating full-text article from 2010 suggests that burden of circulating tumor cells alone is an excellent independent prognostic marker for outcomes in colon, breast and prostate cancer.
Take a good hard look at Biocept, and consider putting some shares in the speculative part of your portfolio. Aegis Capital recently initiated coverage with a buy rating, and a price target of $16, a far cry from the recent $5 share price. Have a go, as I know you will, at Biocept’s recent corporate presentation, where certain particulars are explained in further, if drier, detail. Biocept is certainly the most exciting medical diagnostics company I have ever encountered, and will probably shake up the cancer diagnosis and treatment paradigm like nothing else will. Biocept finds needles in haystacks, but a company this novel, with technology this exceptional, poised for the sort of growth it seems destined for, makes this company a needle-in-a-haystack itself.
This is a discussion topic or guest posting submitted by a Stock Gumshoe reader. The content has not been edited or reviewed by Stock Gumshoe, and any opinions expressed are those of the author alone.
Hail to Gummyland’s Chief Medical Officer KSS for another sensational body of work – well-researched, brilliantly articulated, and artfully framed! At this pace, I figure that by January 2015 we will have acquired enough cutting-edge medical knowledge at GS University (KSS campus) to successfully compete for an internship at Duke or Stanford.
I love your thought process and how you bring things to life. Thanks
LDW
Nice find in a whole different field of biotech Doc. Speculative to be sure but certainly worthy of strong consideration.
Dr. KSS,
Thanks for the great article and clearly elucidating the reasons for purchase of BIOC. Your explanation of the search for circulating cancer cells was fascinating! I’ve always loved science and tech and you make it much more accessible. Thanks again,
Many thanks for your diagnosis Doctor. I note that at Yahoo Finance they speak about BIOC in ‘present’ tense e.g. they SELL bla bla bla. . May I thus infer that FDA has already blessed this product or did I miss something (likely enough)????
Best regards and health.
Ken
Hey Ken, if you read through their 10-K, you will find that they have already been selling their testing services (both clinical and commercial, though I don’t know if they are just the same test for different parties or what). This doesn’t seem to need FDA approval, as they are just analyzing blood samples … they aren’t treating anyone. Here is an excerpt from the 10K:
“Revenue
Revenues were approximately $134,000 for the year ended December 31, 2013, compared with approximately $109,000 for the year ended December 31, 2012, an increase of approximately $25,000, or 23%. The increase was primarily related to clinical trial testing services for our development collaboration program with the Dana-Farber Cancer Institute, partially offset by a decrease in revenues from Clarient. The average price per commercial test decreased from $694 for the year ended December 31, 2012 to an average of $635 for the year ended December 31, 2013. The average price per clinical test was $400 for the year ended December 31, 2013.
Cost of Revenues
Cost of revenues was $2.3 million for the year ended December 31, 2013, compared with $1.2 million for the year ended December 31, 2012, an increase of $1.1 million, or 94%. The increase was primarily related to the volume of clinical tests performed, which increased from zero for the year ended December 31, 2012 to 258 for the year ended December 31, 2013. The volume of commercial tests performed decreased from 130 for the year ended December 31, 2012 to 23 for the year ended December 31, 2013. The net volume increase was due to clinical tests performed under our 2013 development collaboration program with the Dana-Farber Cancer Institute, partially offset by fewer tests performed under our arrangement with Clarient for the year ended December 31, 2013 as compared to 2012. ”
Can anyone clarify the difference between their “clinical testing” and their “commercial testing”?
Thanks for a most entertaining and exhaustive exposition on a difficult subject . I was led to thinking of your analysis of Mauna-Kea Technologies in an earlier post in which you opined that their Cellvizio optical biopsy method would enable ONLY the removal of suspicious nodules and obviate the need for random biopsies. So why is that tech available everywhere else but the US? Is it because that biopsies are the standard of care and lawyers will be lining up to sue if there are misses? A somewhat similar situation probably exists here for Biocept if it is labeled “In lieu of biopsy? Your thoughts?
Kris: To be honest, I think many US places are acquiring Mauna Kea equipment, though admittedly they lag the rest of the world at it. But that very consideration….the sort of almost neurolinguistic programming we have to regard biopsy as the true test and gold standard, yes that will linger for a while. I honestly fear that oncologists, often set in their ways, may be slow to adapt and then, once they adapt, ready to embrace it rabidly once they change their minds. Others are won over by degrees, by gradual persuasion. And lawyers will always have their toes tapping in the background. Ah, the delusions of the US: (1) life is fair, (2) medical outcomes are predictable, (3)medicine is a precise science (it is not precise and only barely science), (4) juries are competent vehicles to try malpractice cases (ha!).
Dr. KSS mentions that BIOC belongs in the speculative part of a portfolio but I like that they do have sales and that insurance companies are reimbursing for their service since it’s less expensive than repeating biopsies. Thomson Reuters has a Strong Buy recommendation on BIOC, I see that some interesting institutions are invested – Vanguard, UBS, Wells Fargo, Citigroup and the Management/Directors are clearly experienced – including the fact that there are more CPA/financial types than I usually see on boards.
Plus, they are growing their list of tests for additional cancers.
Al Sharp RNA interfere ALNY. SMART PEOPLA
Chvostek’s is some what related to Trousseau sign in that you would have to touch a patient or take a BP manually. I’ve seen this a few times when I did not know the Chem panel results, and it has led to serendipitous findings in the patients. Great article as always. Comparing my portfolio of stock recs yours is showing the most green. Certainly some of the best stocks that I would have never found.
Thanks DBMD. I have often found medical students to really wrestle as first years with the seemingly disparate things that they are taught about calcium: that calcium mediates muscle strength and power, but that low calcium (or magnesium) is associated with tetany and muscle tension (for neurologic reasons, not reasons pertaining to the innards of muscle).
This thing has less than 1/4 of the shares outstanding that CLDN has. I wonder how much it will run. Less institutional ownership and insider ownership, so maybe more shares will be “up for grabs” in a way. The stock is shortable, but less than 1% of shares are held short currently.
make that less than 0.1% of shares held short.
Great article Dr KSS. Thanks
Dr. KSS,
Thanks for another journey into the that many of us never would otherwise enter. You make learning fun and profitable. I enjoy reading your articles just as I do some of the finest authors like Isaac Asimov, Mark Twain, and Charles Pellegrino. You are very gifted an I am grateful that we crossed paths here in gummyland. Hope you are feeling better!
Sheesh hasn’t anyone here heard of a “limit order”? Come on.
Half my limit order filled.
What price did you place it at? All of the trades seem to be quite high so far.
Do you think 5.15 is too high Eliott?
Jana, thanks for asking, but I am not experienced enough to give advice. Personally, my buy order is at 4.88 and depending on the price action, maybe I’ll bump it up to 5.08. The 10 day moving average is at 5.04 (and will move up based on today’s action), but I’d rather buy at the 30 day moving average (which is at 4.76, but will move up based on today’s action and the coming days’ action).
Thanks, E. JB
Dr. KSS…on FDA Daily Newsletter…Liver Cancer Drug Fails. Here’s the link:
http://www.reuters.com/article/2014/06/11/lilly-cyramza-idUSL2N0OS0JJ20140611
Best regards, always.
Ken
Thanks Ken. I am long Lilly, but feel they wasted money trialling this, as it had very little theoretical chance of helping hepatocellular carcinoma patients. It is an mAb against VEGF2 receptor, and I am not persuaded that this receptor plays much role in liver tumors, though it does in lung tumors. There is also the issue of portosystemic shunting. You generally don’t get liver cancer unless you have cirrhosis, as the cancer emerges as a consequence of the excessive regenerative activity in cirrhosis. But with cirrhosis, there is intensive vascular shunting around liver, which means that an iv infusion of Cyramza may not have even gotten to the tumor appreciably. A serious approach here would be to embolize the tumor in liver with beads that elute the antibody into the tumor. But Lilly didn’t ask me what I thought.
Gummies…WTH? As Diana said earlier. .. use limit orders when buying something like BIOC. Its up 17% this morning and I bet it’s all gummie-action. Don’t chase this thing at “market” prices.
I’m with you, KennyG. I’m not a very experienced trader and even I know that. With a stock like this with only 4 million shares outstanding, you’re going to drive up the market hugely when using at the market orders.
First thing I learned when I started investing was NEVER use market orders, and I never have. Haven’t had much luck with any of my limit orders lately but that’s OK, I’ve got patience, even though I hate the ‘missed the boat’ feeling.
Up 20% now. I think i’m going to wait until post gummypop.
Me too, Bradley.
Anyone see any news on DRTX? Down 6% ?
Maybe all of these gummies bidding up BIOC and CLDN have been selling DRTX to pay for their orders. IDK. I’ve seen no news, but I’ve been noticing the drop off. Still holding all of my shares.
DRTX up today, and it looks like the CEO added 3K shares to his position yesterday, which is nice
I have a feeling some gummysheep are destined for some gummyshearing on this one. In a very recent parallel example, those who waited for the gummyphfft that followed the gummypop on RGDO got a much better deal. Don’t mean to offend anyone, but honestly, as others have said, limit orders are your friends.
Sometimes that’s the only way people learn. I learned from my mistake on RGDO. And I think maybe people are looking at CLDN and saying to themselves “I missed the boat on that one, I don’t want to miss the boat on BIOC”. Well, CLDN could very easily come down from here, it’s only been a week. I don’t think this lasts for BIOC … they’re a long long way off from being profitable.
I definitely learned with Regado, and a few others I bought at the tip top. I’m holding off for now.
Bcon, I had a limit order that got filled at 15.40 – i’m hoping it’s just a dip…a buying opportunity…
I don’t recall if this one has been discussed, but this article sounds interesting. The company is Flamel Technologies (FLML). They are using current drugs while trying to improve the delivery systems. The article explains why it’s a double in a short period of time – I’m posting for others feedback – I haven’t looked beyond the info in the link here.
http://dailytradealert.com/2014/06/12/this-stock-could-surge-58-in-six-months/
I don’t think that one has been mentioned before. It has a nice looking chart and has a forward P/E of 10.3, according to finviz and yahoo! finance, as it is expected to earn 1.21/share in fiscal 2015. That’s not something you see every day in the biotech world! But who knows how good those analysts’ estimates are. If it doesn’t end up be profitable or not as profitable as expected, the shares will crash massively.
sorry, I said biotech … it’s not a biotech stock, its a pharma stock
Durata is nibbling away at my new position funds…hopefully short lived.
Thanks Elliot. Yes, there is some risk here. Lets see what Dr Kss has to say about the science
I recall this as being one of Motley Fool’s Stock picks several years ago. They were very high on it , obviously.
The above was a reply to post 39 by Bradley about Flamel Tech
Kris, yes — FLML was a pick of Motley Fool Hidden Gems back in the mid-2000s — that newsletter launched in 2003 and it was one of their picks sometime between then and 2007. Don’t know when they dropped it, doesn’t seem to be a current favorite of theirs
Bradley: Personally I would hesitate about being in on Flamel. I am aware of it being touted, of uprevisions of estimates, possibly even some insider buying, but there is not much compelling about this story. This company’s work is very applied and very derivative….a bunch of knock-off me-too drug delivery modalities, none of which are truly novel or clever, and none of which really represent big therapeutic inroads. They are adjustments to, minor refinements of, existing methods. If shares appreciate, I would surmise that their horizon for doing so is constrained. For me, I would see no reason to be in the stock. It is almost too boring to justify following it, as it has not done anything actually original.