
The term “the duration” immediately recalls the Second World War. Nobody had any idea when it would be over, and so discussions of a lot of World War II-related events and conditions prominently featured the phrase “for the duration” – as in great numbers of combat fatalities would continue to be reported for the duration, and gas rationing would continue for the duration. That basically meant that these conditions would continue as long as they continued, but nobody really knew for how long.
The same thing is the case with COVID 19. It is the dominant reality for the duration, which means it will go on as long as it goes on. How long that will be, no one really knows. But perhaps there are signs and indications that we can look at today as a way of bringing our speculations a bit more into focus.
What makes for hot news is when there are upsurges in new COVID 19 cases, whether these take place in one neighborhood in Brooklyn, in an entire state in the midwestern US, or the whole subcontinent of India. Information about how an upsurge is controlled is, for some reason, not so hot. But if we’re keeping an eye out for relevant developments in this pandemic, the not-so-hot news can be just as important, and perhaps more important.
For a start, let’s look at how two very different places managed, or attempted to manage, the coronavirus.
Sweden and Arizona versus COVID 19
Sweden pinned its hopes on herd immunity. The idea was that as more people become infected and (hopefully) recovered from the disease, and therefore acquired a degree of immunity, there would be a decreasing number of people in the community who would spread the infection. The epidemic in Sweden would therefore diminish along with the proportion of potential disease spreaders. But for this to happen in reality, there either has to be an effective vaccine or a very high fraction of the population has to develop immunity due to having had the disease itself. In terms of defeating COVID 19, this was an optimistic assumption – an assumption that took for granted that many, many people would acquire the infection, and that perhaps a few of these unfortunates would die, but that the COVID 19 plague would go away. That assumption did not work out.
At this point, Sweden has over 100,000 cases and nearly 6,000 COVID 19 deaths. Its immediate next-door neighbor, Norway has about 16,000 cases and fewer than 300 deaths. Sweden’s population is about double Norway’s, but Sweden’s infection rate is triple Norway’s and its death rate is ten times higher.
The inhabitants of the two nations are similar, and both nations have excellent health-care systems. The chief difference is that while Norway put into practice strict preventive measures such as social distancing and masks, Sweden did not. Some individuals in Sweden took precautions as a matter of individual choice, but the government made no move to enforce or even encourage these precautions. The results are evident from the comparable infection and death rates.
Now let’s take a look at Arizona. When the coronavirus started to emerge as a serious threat, Arizona imposed business closures and stay-at-home orders similar to those in many other states. But as there began to be hints that the threat from the virus might be abating, Arizona’s Governor Doug Ducey, yielding to pressure to re-open the state, did not continue these closure orders beyond May 15th. Whereupon daily diagnoses of COVID 19 took off like a rocket, climbing by a factor of ten over the following six weeks. That surge reached its crest around the end of June, at which point Governor Ducey reimposed those previous protective measures. And from that point, the number of new infections plummeted, so that by early August, new infections were down to the levels seen in early May.
The graphic below, from the Morbidity and Mortality Weekly Report (part of the CDC) tells the story.
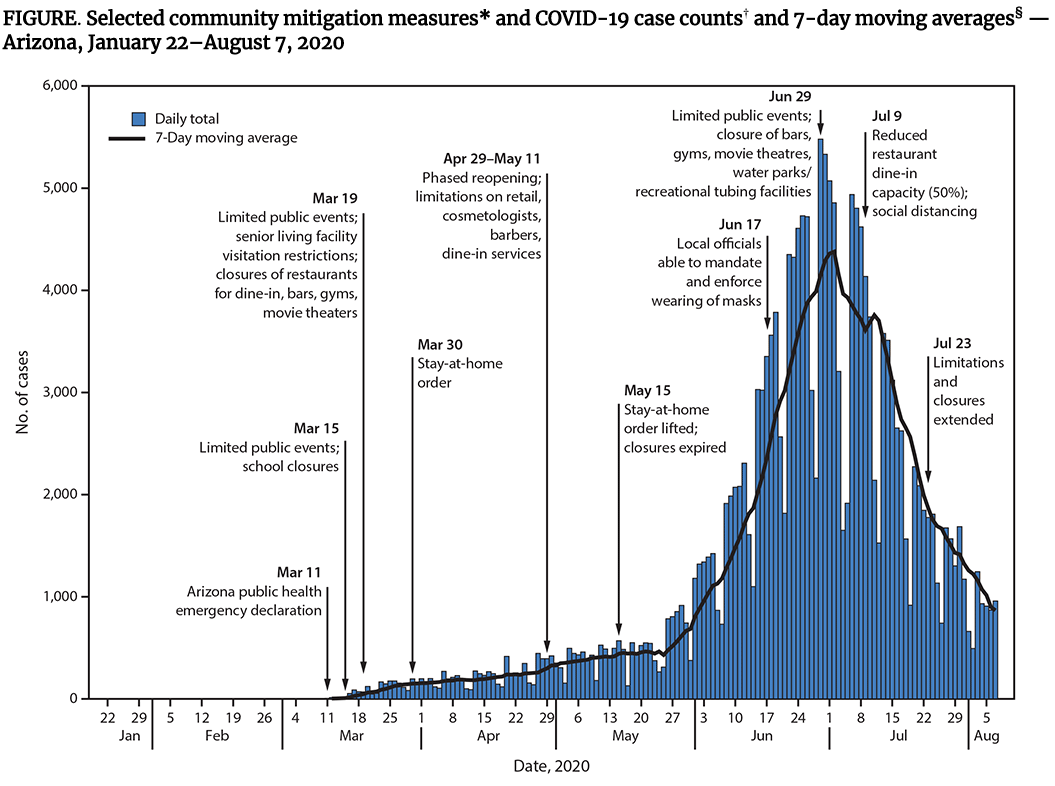
Certainly, based on those data, the protective measures that were reimposed in the middle of June are what did the trick.
The moral of this story, if it needs to be pointed out, is that simply letting herd immunity develop on its own causes severe harm to many, many people. It is a deadly strategy.
How to get to herd immunity
The results of Sweden’s reliance on herd immunity should not discredit herd immunity as an effective way of curbing the spread of a communicable disease. The question is, how is herd immunity achieved? Sweden apparently thought that it would come about naturally as more and more people got infected and recovered, having acquired some immunity. This may have led to the conclusion that the best way of achieving this goal was to do little or nothing to prevent the spread of infection. Historically, some epidemics may have been slowed in exactly that same way. At the time of the 1918 flu pandemic, there was no flu vaccine, and it was largely herd immunity that finally slowed it down. However, other devastating infectious diseases have effectively been stopped by means of vaccines, smallpox and polio being prime examples. And, of course, widespread vaccination is the prime means of getting to herd immunity.
A group of three eminent medical scholars have proposed an alternative method of attaining herd immunity in a document entitled “The Great Barrington Declaration,” which reportedly has been signed by over 90 clinicians and 300 medical workers. They propose a strategy which they suggest will offer maximum protection for persons most at risk of serious infections and death, while permitting people who are at lower degrees of risk to continue relatively normal lives. Here’s an excerpt from that document:
“Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice.
“Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.
“The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.
“Those who are not vulnerable should immediately be allowed to resume life as normal. Simple hygiene measures, such as hand washing and staying home when sick should be practiced by everyone to reduce the herd immunity threshold. Schools and universities should be open for in-person teaching. Extracurricular activities, such as sports, should be resumed. Young low-risk adults should work normally, rather than from home. Restaurants and other businesses should open. Arts, music, sport and other cultural activities should resume. People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity.”
… but I strongly disagree with that position
Having quoted extensively from the Great Barrington Declaration, I needed to emphasize my disagreement, in bold italics.
"reveal" emails? If not,
just click here...
There’s no question that the lockdown caused serious problems to the economy and an enormous disruption of people’s lives. But the authors of this declaration seem to ignore the really horrendous effects on the health and lives of those persons whom they describe as “not vulnerable.” In my view, calling them “not vulnerable” is a flat-out falsehood. Younger people can and will get sick, and some of them will die. And, on top of that, younger people and quite young children can pass the coronavirus infection on to those same susceptible older people. Kids can infect and essentially kill their grandparents. What the Great Barrington Declaration proposes is to trade the lives and health of some for the benefit of others.
On October 15th, a letter was published in The Lancet, signed by 80 medical and scientific professionals, that opposed that proposal in the most emphatic terms:
“This is a dangerous fallacy unsupported by scientific evidence.
“Any pandemic management strategy relying upon immunity from natural infections for COVID-19 is flawed. Uncontrolled transmission in younger people risks significant morbidity and mortality across the whole population. In addition to the human cost, this would impact the workforce as a whole and overwhelm the ability of health-care systems to provide acute and routine care. Furthermore, there is no evidence for lasting protective immunity to SARS-CoV-2 following natural infection, and the endemic transmission that would be the consequence of waning immunity would present a risk to vulnerable populations for the indefinite future. Such a strategy would not end the COVID-19 pandemic but result in recurrent epidemics, as was the case with numerous infectious diseases before the advent of vaccination. It would also place an unacceptable burden on the economy and health-care workers, many of whom have died from COVID-19 or experienced trauma as a result of having to practise disaster medicine.”
The Great Barrington Declaration also provoked stern rebuttal from the Infectious Disease Society of America (IDSA), which issued a statement to the effect that they “strongly denounced” that strategy, saying that “it comes without data or evidence.”
And here’s a quote from Dr Anthony Fauci:
“Anybody who knows anything about epidemiology will tell you that this is nonsense and very dangerous, because what will happen is that if you do that, by the time you get to herd immunity, you will have killed a lot of people – that would have been avoidable.”
Just to be really, really clear, what these people are denouncing is the concept of deliberately trying to get to herd immunity by letting increasing parts of the population get infected with the coronavirus. Arriving at herd immunity by means of a vaccine, on the other hand, is generally agreed to be an objective of the greatest importance.
So, how are we doing in the quest for vaccines?
In spite of repeated proclamations from On High that there would be a vaccine widely available by November 3rd, or at least before Christmas this year, it doesn’t look as though that’s going to happen. Just a few days ago (as I write this), Dr Moncef Slaoui, who is the co-chair of Operation Warp Speed, made a statement that the government agency (which had been organized to accelerate the vaccine process) was urging manufacturers not to apply for emergency use authorization (EUA) until they had enough doses of their vaccine on hand to vaccinate a meaningful portion of the population.
Operation Warp Speed, as perhaps you know, is a $10 billion initiative, whose central goal is to develop, produce, and distribute 300 million doses of an effective vaccine by mid-January of 2021. The organization is quasi-military – more than 60 military officials are on the organization chart. It’s acknowledged that the military have no knowledge of the science of vaccine development. But they have already helped prop up more than two dozen vaccine manufacturing facilities by flying in equipment and raw materials from all over the world. They have also set up significant cybersecurity and physical security operations to ensure that any eventual vaccine is guarded very closely from possible intervention by forces that may not want the US to be the first nation to have an effective vaccine.
Dr Slaoui has suggested that FDA approval of a vaccine that was not actually available at that time would be “a major disappointment.” Polls have shown that many Americans are mistrustful of vaccine development being rushed and inadequately tested; as many as 50% have said that they would refuse a vaccine produced under those circumstances.
The FDA has been trying to clarify the regulations under which a vaccine would receive an EUA. The agency just recently posted their updated safety standards in advance of a meeting of the advisory committee which advises the FDA on safety standards, scheduled for October 22nd. The FDA wants vaccine manufacturers to collect safety data on at least half of the trial subjects for two months after they have received their second dose of a two-dose vaccine.
Of the current frontrunners in the vaccine race, the only one that uses a single-dose vaccine is the Johnson & Johnson candidate. But J & J just recently interrupted its Phase 3 clinical trial due to a “safety incident.” Currently, 60,000 persons are enrolled in the trial, which remains on hold. J & J declined to provide further details, but pointed out that it is not apparent in cases like this whether the adverse event took place in the treatment arm or the placebo arm. Even though the trial has been interrupted, it continues to be blinded, therefore no one knows the status of an individual subject.
At this point Pfizer in collaboration with BioNTech are the leaders of the pack. Their vaccine is a messenger RNA formulation. These are much quicker to be developed, particularly in the early stages. They recently got FDA approval to include subjects as young as 12 years old in their safety trials. Most other vaccine trials are not enrolling any subjects under the age of 18. As of mid-September, Pfizer/BioNTech announced that only 12,000 of the projected 30,000 subjects had received a second dose of the vaccine, meaning that they would have the necessary safety data to apply for an emergency use authorization by mid-November at the earliest, since it usually takes about two months for vaccine-related adverse events to emerge. Data on the efficacy and immunogenicity of the vaccine will follow. Some estimates have put the time frame for such data as mid-January to mid-February of 2021.
It is not clear at this point what standard the FDA will use to judge the effectiveness of vaccine candidates. A potential standard that has been aired and discussed, mostly critically, is that to receive any kind of approval, a candidate would need to demonstrate that in at least half of the vaccinated trial enrollees, the COVID 19 symptoms would be reduced by about half. This “half of a half” standard may have some merits, particularly when it comes to speed of arriving at a decision and getting a vaccine out in quantity, even if it is perhaps only somewhat effective.
As you can see from the table below (which appeared in the October 13th issue of Lancet), there are currently nine Phase 3 clinical trials in COVID 19 vaccines underway. The other presumed front-runner, Moderna, based in Cambridge, MA, has not received FDA approval for its candidate vaccine. Nonetheless, they have announced plans to make between 500 million and 1 billion doses of their vaccine per year, when it gets approval, whenever that might be. It has been pointed out several times, including in past Doc Gumshoe pronouncements, that Moderna has not yet brought a vaccine for any disease through the approval process.
| Phase 3 trials Developer | Platform | Location |
| AstraZeneca; University of Oxford (30 000 participants) | Chimpanzee adenovirus (ChAdOx1/AXD1222) | UK; India; Brazil, South Africa; USA |
| Moderna; National Institutes of Health (30 000 participants) | RNA (mRNA-1273) | USA |
| Pfizer; BioNTech (44 000 participants) | RNA (BNT162b1 and BNT162b2) | USA |
| The Janssen Pharmaceutical Companies of Johnson & Johnson (60 000 participants) | Adenovirus serotype 26 vector (Ad26.COV2.S) | USA; Argentina; Brazil; Chile; Columbia; Mexico; Peru; Philippines; South Africa; Ukraine |
| The Gamaleya National Research Centre for Epidemiology and Microbiology; Academy of Military Medical Sciences (40 000 participants)
| Adenovirus serotype 5 vector and adenovirus serotype 26 vector (Sputnik V) | Russia |
| CanSino Biologics; Academy of Military Medical Sciences (40 000 participants) | Adenovirus serotype 5 vector (Ad5CoV) | China; Pakistan |
| Sinovac Biotech (9000 participants) | Inactivated virus (CoronaVac) | Brazil; Indonesia |
| Sinopharm; Wuhan Institute of Biological Products (21 000 participants) | Inactivated virus | The United Arab Emirates; Bahrain; Peru; Morocco; Argentina; Jordan |
| Sinopharm; Beijing Institute of Biological Products (5000 participants) | Inactivated virus (BBIBP-CorV) | The United Arab Emirates |
The AstraZeneca trial is on hold in the US because of an adverse event which took place in the UK. As mentioned earlier, the Janssen/J & J trial is similarly on hold due to an adverse event in one participant.
In addition to the nine Phase 3 trials shown above, 21 Phase 1 and Phase 2 trials are now underway. Inovio, which was one of the first pharmaceutical companies to announce that they were developing a vaccine against the coronavirus, is only now in Phase 1 trials for its candidate vaccine.
Also in Phase 1 are two major contenders – Sanofi and Merck, both of whom entered the race relatively late. Sanofi is developing a messenger RNA vaccine in collaboration with Translate Bio of Lexington, MA, relatively small biotech that has been working with mRNA for the past ten years. Phase 1 trials with this vaccine are expected to start in November. John Shiver, head of vaccine R& D for Sanofi, projected that the earliest their vaccine might be approved, if it has been shown to be safe and effective, would be the second half of 2021. The partners believe that they can make between 90 and 360 million doses of a mRNA vaccine against the coronavirus before the end of 2021.
Sanofi has a second vaccine in development. This one is a recombinant protein vaccine, which is used with another compound to boost the response of the immune system. The second compound is made by Glaxo SmithKline. Currently, a Phase 1/2 clinical trial involving 440 subjects is underway. Safety and preliminary immunogenicity data may become available by the end of December, according to John Shiver. Sanofi/GSK are currently manufacturing doses of the actual vaccine, and expect to have 100 million doses by that time, in case the FDA issues an emergency use authorization that soon.
Sanofi’s recombinant protein vaccine uses the same platform as Sanofi’s Flublok vaccine, which may be an advantage, since regulators are already familiar with the platform’s mechanism, and thus may go through the approval process somewhat more quickly.
One of Merck’s two vaccine candidates also employs a platform that the regulators understand. The vaccine is made by combining genetic material from the coronavirus, SARS-CoV-2, which causes COVID 19, with a virus that can infect humans without making them ill. This virus, the vesicular stomatitis virus (VSV), has been abundantly shown to trigger a robust immune response in humans. The VSV virus was fused with the virus that causes Ebola, producing a vaccine that has been reported to have outstanding efficacy. An unusual feature of the VSV Ebola vaccine is that it works equally well in the elderly as in younger people. If the COVID 19 vaccine had features similar to the Ebola vaccine, that would be a marked advantage.
A second vaccine is being developed by Merck in collaboration with their newly-acquired subsidiary, Themis BioScience. This candidate uses an attenuated measles virus as the vector for the coronavirus genetic material to the human immune system. As yet, no licensed vaccine uses this platform, but other similar vaccines under development are showing promise.
In all, 30 COVID-19 vaccine candidates are at some stage of development. It’s highly likely that some of these will receive emergency use approval, and some may even receive full FDA approval. Some of these will offer only partial protection, and offer protection to some persons but not others. But some vaccines may be highly effective, and some vaccines may protect the great majority of individuals. With a disease that has attained pandemic proportions – at this moment, nearly 40 million cases globally, and well over a million global deaths – even a half-way benefit to half the population is better than nothing, especially if more robust and broadly effective vaccines come along.
Speaking now for myself, if the first vaccine that came along was one of those half and half deals, and I was deemed eligible to receive it – and if it had received EUA from the FDA – I would go ahead and get myself vaccinated. And then, when a better one came along, if there were no contraindication, I would get myself vaccinated again. My guess, based on what we know up to this point about the mutability of the coronavirus, is that there will be no single vaccine that is good for a lifetime of immunity. Whether it will need to be repeated annually, like the flu vaccine, no one yet knows. For the duration, we will need to base our decisions on whatever we know at this point.
Other COVID-19-related topics
Scientists and the medical community in general have now been working with and investigating the coronavirus for almost a year. They have learned a good deal, and although quite a lot about the coronavirus and the disease (or diseases) that the coronavirus causes is still poorly understood, what they have learned will likely provide avenues that lead to effective ways of treating and managing this disease.
Here are a few of the COVID-19-related topics that Doc Gumshoe will take up in the next epistle:
- The relation between virus load and the severity of symptoms;
- The increasing range of treatment options for COVID-19 that, while not offering a cure, do address patient symptoms;
- The relationship between obesity and COVID-19 severity;
- The neurologic symptoms that COVID-19 produces, particularly in young people;
- How the coronavirus affects persons with different blood types;
- The clinical effect of coronavirus antibodies;
- Cardiovascular effects of COVID-19
- The disruption of the renin-angiotensin system (RAS) as the mechanism through which the coronavirus wreaks its devastation.
* * * * * * *
And, in the intervals when I turn my attention away from COVID-19 (believe me, this takes an effort of the will), other topics attract me. For example, one that was suggested by one of the Gumshoe faithful was the possibility that memory loss was mostly due to bacteria. Can this be true? Doc Gumshoe will try to find out. In the meantime, keep those stimulating comments coming at me. Best to all, Michael Jorrin (aka Doc Gumshoe)
[ed. note: Michael Jorrin is a longtime medical writer (not a doctor), who I dubbed “Doc Gumshoe” many years ago — he writes health and medicine-focused columns for our readers a couple times a month, and though he does not generally cover investment ideas he has agreed to our trading restrictions. You can find his past columns here.]
DocGumshoe may want to include some mention of ‘challenge’ trials, what they are, how they’re supposed to work and the ethical issues ?
The British Govt has just awarded a conditional contract to OpenOrphan (LSE : ORPH) , where I’m invested.
Yes, the Brits are planning a challenge trial. A challenge trial, in case you don’t know, is a clinical trial in which doses of the infectious agent – in this case the coronavirus – are given to volunteers who have received a vaccine to attempt to determine if the vaccine protects them from the infection, and if so, how well. Needless to say, this is a delicate issue. Challenge trials have been done where the vaccine is against an infection that has a fairly reliable treatment available, so that if the vaccine doesn’t work and the human subject gets infected and develops symptoms, there’s a way to deal with it. But, as you know, there is no reliable treatment for the coronavirus infection. In the case of the coronavirus, the scientists will initially try to determine what’s the least dose that causes an infection. They won’t be hitting these trial volunteers with a does large enough to cause dangerous symptoms – or at least, that’s what they hope.
Lots of questions will still remain unanswered. If the vaccine is shown to protect subjects from a small dose of the virus, will it similarly protect real-life persons from a larger dose – say, directly taking in droplets from a cough or a sneeze? And if it works reasonably well in the healthy young volunteers who will participate in the trial, how well will it work in oldsters and people with significant comorbidities?
As with many issues around COVID-19, we’ll just have to wait and see.
“…as you know, there is no reliable treatment for the coronavirus infection…”
Sure there is. It’s called vitamin D.
Lots of credible studies on line that lend support to this contention.
(I didn’t realize until after posting this comment that I was replying to Doc Gumshoe himself. At least the edit feature allows me the chance to clarify) !!
Hydroxychloroquine + zinc + azithromycin appears to be very effective when used at conventional doses and when used early in the disease. https://www.sciencedirect.com/science/article/pii/S0924857920304258 When hydroxychloroquine is used at very high (perhaps even toxic) doses, as was done in a couple of high-profile trials this year, or on patients whose illness is already advanced, it doesn’t work.
They never Isolated the Virus,,,,,,Look at Netherlands research as well.,
I am more on the side of covert 19 .
Thanks
Good point here, I hope they all listen because the ones here with covert stocks can be hurt very roughly if they don’t watch out. Do your own DD I would say.
After some 50+ years since the Flu (H3N2) outbreak that did not close down the country, even though thousands of lives were lost, there is still no single vaccine that kills all strains because the virus continually mutates.. Much like the common cold.
Covid 19 is another strain of flu-like Cov 2 which killed thousands in SE Asia. SARS was beaten by the effects of Herd Immunisation as there was never any vaccine produced for it. The best way to beat such a virus is by allowing the less vulnerable, to develop in their own auto immune systems, an antigen to kill it or downgrade its effects so that it mutates into a less infectious virus that will not affect the now vulnerable.
Recent figures from the Official National Statistics in the UK state that the deaths due to Covid 19 are 24th in the league of the Causes of Deaths in the country. Flu and pneumonia sit in eighth position and the Number One killer is Dementia.
It’s not the number of those positively tested (Or the false positives) that should concern, it is the number of deaths caused SOLELY by the Covid 19 Virus and they have been falling regardless of the direct actions. Check out the low Stats from knowledgeable and experienced SE Asia compared with the RoTW.
There is no doubt that promoting herd immunity is the basis for the increased mortality rate in Sweden. Unfortunately, that is because it is relatively easy to connect death with Covid statistically (even though this is sometimes carried to an extreme (motorcycle death listed as Covid, hospitals being told by CFOs to note Covid as cause of death for reimbursement purposes, etc.). What is not being weighed, because there are no immediate visible effects, are the long term repercussions of shutting down the world that are throwing people out of work and into a poverty which no government can afford to keep subsidizing, and the mental health costs of isolation of seniors, many of whom would choose to risk getting infected rather than spending their remaining years in imposed isolation. There is no simple solution but the fearmongering is causing as much harm as the illness. A little more press about how 80% of people who get Covid will be just fine would go a long way to improving mental health and reduce suicides rather than the anecdotal reports of a young person dying (which happens every day from innumerable causes) or someone having long term ill effects from the virus, which also happened everyday from some malady or other.
Well done summary with great clarity. Congrats. But Doc Gumshoe’s perspective at one point in time on a complex subject. I was impressed with Moderna which has multiple phase 2 and 3 studies going including the one on Covid. I bought a basket of companies including Sanofi, J&J AZN,PFE, and Moderna. Rarely is there a time when the world is hoping and now is that time.
There was a NY times piece six weeks ago ( approx ) about a study in NJ, NY & Nevada that showed a 90% false positive test result from CVR testing method. Has anyone else read this, if so, can someone comment on this? In my town several people have tested positive and their spouses sleeping in the same bed the entire time never got it.
At low incidence rates (which is where we are now in most parts of the world) even a small false positive rate on the test becomes very important; at zero incidence, 100% of the positive tests are false . Here is a paper from a lab at Addenbrookes’ Hospital in the UK https://www.clinicalmicrobiologyandinfection.com/article/S1198-743X(20)30614-5/fulltext#%20
where in June-July they found that 44% of their positive tests were false positives, in the sense that the positive result could not be replicated on retests (usually 2 retests).
…and another lab reporting that their tests were 65% false positives over the same period, again based on whether or not a retest confirmed the result https://www.bmj.com/content/369/bmj.m1808/rr-22
PCR tests are a powerful tool but they need to be used sensibly. If they are used to test large numbers of asymptomatic people when the disease prevalence is low, there are likely to be a lot of false positives.
so, why do you think one group of doctors is right and the other wrong? I think it more likely suggests “we don’t know for sure”. And, there has never been a vaccine developed for any of the family of corona viruses ever, let alone in record time (months versus years).
You’ve strongly disagreed with herd immunity because, “Younger people can and will get sick, and some of them will die.” Seriously, please start using actual data instead of generalities that allow you to hide behind a lack of facts. The CDC estimates “younger people” (less just say under 20) have roughly a 1 in 10,000 chance of dying…IF they contract the disease. Who knows what this value would be if co-morbidities in the younger people was stripped out of this estimate. Certainly even lower.
Let me use more data, straight from the CDC website (I encourage each person to check this themselves). The mortality rate for those who contract the virus is estimated to be 0.27% across the FULL population of the US. I also took flu mortality calculations for the 2 last years of final data available (2017, 2018) and found that to be 0.25%.
These numbers are not offered up directly; you have to calculate them based on infection fatality ratios, estimated asymptomatic percentages and total fatalities to get these numbers. So I did.
The mortality rate appears to be “flu-like”, including how it impacts the population by age.
Disagree with my numbers if you want, but you better use statistics to do so. I’m an engineer, and I “strongly disagree” with people throwing conclusions around without providing the basis for those conclusions.
Your statements on how Arizona addressed Covid do NOT take into account that the sharp spike up and then DOWN in cases may actually indicate herd immunity being roughly achieved in the primary population centers of the state. You completely MISSED the possibility of awaiting additional data from the state to show if that herd immunity is actually a viable theory.
Your bias appears to be giving you blind-spots with this topic.
Please clarify:
“The mortality rate for those who contract the virus is estimated to be 0.27% across the FULL population of the US”.
Are you saying that 0.27% of those infected die, or that
of the FULL population of 328.2 million, 0.27% die.
I’m genuinely confused.
Hi Jim T. I’m saying the CDC numbers estimate 0.27% of people who get infected with COVID die. That is the mortality rate for this virus, again, according to the CDC. These n umbers are completely based on CDC estimates and are accurate as of beginning of October.
I think it’s self-evident that lock-downs slow the spread, the debate is really at what cost, and to what extent are we preventing infections vs. prolonging the pain.
Some of the lock down costs economically, and societal are probably cumulative, while the benefits of flattening the curve are diminishing – at what point does the cost exceed the benefit?
Also, we’re assuming the vaccine will change everything, but what if a vaccine is say only 40% effective, do we stay locked down because “younger people can and will get sick, and some of them will die. ” Unfortunately that kind of specious argument can be used for anything.
https://www.youtube.com/watch?v=eXWhbUUE4ko
Another valid perspective: https://www.lewrockwell.com/2020/10/joseph-mercola/coronavirus-fraud-scandal-the-biggest-fight-has-just-begun/
Hello all,
I live in Brazil and work in Alaska. In Alaska I am the Captain of a large fishing vessel. We had a mate with Covid in January of this year. This was before Covid was a known issue. He infected everyone that worked in close contact with him except for myself. We know it was Covid because of his symptoms including loss of taste and smell.
At the time I was taking heavy doses of vitamin D. I have heard of other people that think Vitamin D helps in fighting off the virus. Sunshine is a natural provider of vitamin D. It is worth some further reaserch.
Here in Brazil there is a Vaccine from China. The doctors and Gov. of Sao Paulo State SP. want to use it but Bolsenario, the President is resisting its use. I suspect China wants to use the Brazillians to test the vaccine. I am curious if the vaccine was tested in China.
William Fitzgerald
The increasing range of treatment options for COVID-19 has a total of 319 trials as of this date.
Why not separate treatments that are based on previously approved prescribed medications or natural formulas and use them immediately. Vitamin D, Zinc, Famotidine, and Aviptadil have shown signs of being effective against Covid-19. For anyone that contracts Covid-19 to have to wait 8 or 9 months to be allowed these “Do no harm” possible remedies as a choice as a possible intervention on their behalf would not be fair. IMHO
Why not release results on this group? Or any group of treatments that are being used that bring the death toll down. Allow those most in need “The Right To Try”.
NeuroRx and Relief announce topline efficacy data from patients treated with
RLF-100™ (aviptadil) under the U.S. FDA Expanded Access Protocol authorization
for respiratory failure related to critical COVID-19
– RLF-100™ therapy associated with a 9-fold increased probability of survival
and recovery from respiratory failure in an open-label, prospective study
– Top-line data from randomized, placebo-controlled Phase 2b/3 trial expected
this quarter
PR Newswire
GENEVA and RADNOR, Pa., Oct. 13, 2020
GENEVA and RADNOR, Pa., Oct. 13, 2020 /PRNewswire/ — RELIEF THERAPEUTICS
Holding AG (SIX: RLF, OTCQB: RLFTF) (“Relief” or the “Company”) and NeuroRx,
Inc., today announced topline results from 45 patients assessed in an
open-label prospective study where 21 patients admitted to an intensive care
unit (ICU) with critical COVID-19 and respiratory failure were treated with
RLF-100™(aviptadil) and compared to 24 control patients treated in the same
setting. All patients had severe comorbidities that rendered them ineligible
for the ongoing randomized controlled phase 2b/3 trial being conducted to
ascertain safety and efficacy of RLF-100™, and all patients were deteriorating
despite treatment with approved therapies for COVID-19.
(PRNewsfoto/NeuroRx)
Overall, 81% of RLF-100™-treated patients survived beyond 60 days, compared to
17% of control patients. Patients treated with RLF-100™ demonstrated a 9-fold
increased probability of survival and recovery from respiratory failure, with
a high degree of statistical significance. Statistical analysis was performed
by Prof. Phil Lavin, FASA, FRAPS of the Boston Biostatistical Research
Foundation.
“We are encouraged by these initial results in highly comorbid patients with
COVID-19 respiratory failure, and we are pleased that the majority of these
patients have returned safely to their families. We look forward to the
upcoming results from the randomized, double-blind, prospective trial in less
severely comorbid patients for confirmation of these results,” said Jihad
Georges Youssef, MD, section chief of General Academic Pulmonary Medicine at
the Houston Methodist Hospital, who serves as the study’s principal
investigator at Houston Methodist and also serves as national co-chair for the
ongoing randomized controlled trial
Thanks for those leads – I’ll follow up!
“THAT”S WHAT I’M TALKING ABOUT” This is how we can win!
One drug at a time at ‘Warp Speed’ 3 or 4 therapeutics then a vaccine or two.
319 treatment trails and 213 Vaccine trails. An easy read—- https://covid-19tracker.milkeninstitute.org/
Thank you Michael Jorrin for your reply.The US Food and Drug Administration (FDA) has given full approval to the first drug to treat COVID-19. The antiviral Veklury (remdesivir, Gilead Sciences) received approval on 22 October to treat older children and adults who are hospitalized with COVID-19.
I would add monolaurin to your list. It’s safe and available over the counter. Monolaurin is made from coconut oil, and it’s essentially a concentrated dose of lauric acid, which dissolves the lipid coating of viruses that have a coating. All coronaviruses have a lipid coating.
Another plant-based treatment is the seed called black cumin (nigella sativa), or its oil, which has a very long history of treating respiratory ailments, as well as other illnesses.
An herbalist I know claims success with holly leaf, angelica, and pine needles, and recommends elder flower or elderberries as a preventive.
I’ve been taking Vitamin D every day, and take Vitamin C several times a week. If I begin to get cold-like symptoms, I use zinc lozenges, black cumin, elderberries, and flushing my sinuses with salt water in a neti pot.
This Dr. Gumshoe article is one of the best that I have read on the topic of Covid-19 and where we are in terms of finding a cure or a slow-down of the symptoms associated with it. I would take this seriously. I’m invested in some of these companies and believe a couple more appear to make sense based upon the odds and the diverse methods of approaching an effort of locating pharma held in reducing and/or eradicating the effects of this virus pandemic. AF
Dear Doc,
you seem to repeat the NYT mantra, comparing Sweden efforts to Norway. Norway is more sparsely populated, a better comparison would be with a larger European country, like Italy or France, which have chosen a more stringent policy of restrictions.
At this link you can find the “excess deaths” calculations by The Economist.
https://www.economist.com/graphic-detail/2020/07/15/tracking-covid-19-excess-deaths-across-countries
What I find difficult to understand is that people against the Great Barrington Declaration claim that it “comes without data or evidence” forgetting to say that their own strategy has no data nor evidence. Better yet, we do know that if we locked down all the people in the world ,the number of contagions and deaths would decrease dramatically but we also know that’s an impossible policy to implement.
I also find that nobody has really grasped the enormity of the side effects of this prolonged restrictions. I wish some economist would attempt to calculate not only the economic costs but also and mostly the costs in uncured diseases, untimely deaths, and the general malaise.
Most of the deaths happened in the beginning.Now doctors know how to better tackle the virus so maybe the Barrington people should be given some attention.
Following is some data, updated to about the middle of September, comparing Sweden results with Italy’s (which has had a strict and long lockdown)Questo è il sito ufficiale che piú ufficiale non si può…
First of all, here’s the official source
https://covid19.who.int/region/euro/country/it
Sweden (no lockdown, etc.)
Population 10.230.000
Total cases. 86505
Total deaths 5846
Percentage deaths/cases 6,75
Percent. deaths/population 0,057
Percent. cases/population. 0,84
Italy (Full lockdown, restrictions, etc.)
Population 60.360.000
Total cases. 286.297
Total deaths 35.603
Percent. deaths/cases 12,4
Percent.. deaths/population. 0,058
Perc. cases/population 0,47
Italy has had more deaths relative to the number of cases, which is explained by it being the first country to be badly hit when nobody knew what to do (and some doctor admitted that they were rushing too many patients into ventilators only to see them die…) while the percentage of cases , relative to the population is almost double for Sweden (reflecting their more liberal policy ).
Most important however, at least by my conservative attitude, in the percentage of deaths which is identical for the 2 countries and makes me question if those lockdowns are justified.
“Italy has had more deaths relative to the number of cases, which is explained by it being the first country to be badly hit when nobody knew what to do (and some doctor admitted that they were rushing too many patients into ventilators only to see them die…)” Is it recorded that 80%, yes, 80% of those first contractors of Covid that were put on ventilators died? What is the current percentage of ventilator usage and mortality rate?
I don’t know the percentage, quite small, however. I remember the loud requests by the press, politicians, etc to increase the number of ventilators. Lombardy even built a brand new site with lots of ventilators…now sitting unused.
As someone said, in a crisis you need to be seen doing something, anything.
And someone made, and is making , some good money. Is that why the G.B. D. is not well received by so many?
Comparing Sweden and Italy is not valid – when the coronavirus hit Italy, the world was totally unprepared. When Italy instituted containment measures, both the infection and fatality rate dropped dramatically. By the time the coronavirus started to manifest in Sweden, effective containment measures were pretty well understood and put into effect in several countries, Norway being one. The UK was not nearly as thorough with those measures as other EU nations, and fared poorly as a result.
“When Italy instituted containment measures, both the infection and fatality rate dropped dramatically” – which is what flu viruses do on their own with no lockdown, and what COVID did in the non-lockdown countries (Sweden, Belarus, Nicaragua, Tanzania, effectively Burundi) and the light lockdown countries (Japan, Uruguay, South Korea). Governments seem to be claiming credit for a natural process.
The UK fared better than Spain and Belgium, which were both more “thorough”, and worse than Denmark which had a relatively mild lockdown. There have been claims that the UK began its full lockdown “late” but the virus arrived in the UK later than most other European countries. Germany also locked down late and had a mild outbreak.
Lots of good counter-points made in these articles, MJ (“doc”). Truly I hope you are following up the stats presented and the leads given to more fully explore the other side of this argument you presented above.
I truly believe the facts present a very different picture for people to consider than this narrative of lockdown until a vaccine is ready. The multitudinous costs of such a policy are only beginning to become more clear.
Doc Gumshoe’s discussion of the Swedish experience assumes that differences in mortality between countries are largely a result of government policy, with no confounding factors. That’s possible, and it’s what governments would of course like you to think, but it’s still a bold assumption. The countries that have been included so far in the Short Term Mortality Database on mortality.org indicate that all the countries that had high COVID mortality had a period of significantly below-trend mortality in the year or two before the pandemic, while the countries that had low COVID mortality had average to high excess mortality over that period. The people in Sweden who died from COVID were likely mostly people who would have died in 2019 had that been a more normal year.
Likewise South Korea’s “success” with the pandemic likely had little to do with track and trace, which is not really practical in a disease that for most people is so mild you have to be tested to see if you have it, and where clinical false positive rates can be as high as 40% and clinical false negatives run at 20% even at the peak of infection. The Koreans had high excess mortality in the preceding couple of years, which removed the vulnerable population; of course, the people who have recently become concerned about people dying didn’t care about those deaths, because they weren’t COVID.
Those who criticise Sweden also need to explain Peru, where despite what was likely the world’s earliest, harshest, most mask-wearing lockdown, COVID mortality per capita is the highest in the world, with non-COVID deaths also well above trend this year. Compare that to other Latin American countries that had mild or no lockdowns and few deaths – Uruguay (mild lockdown), Nicaragua (no lockdown), even Brazil where there were patchy lockdowns and little sign of excess deaths, suggesting that they might even be over-attributing deaths to COVID.
We need to be consistent; if the Swedish COVID deaths that just brought their overall death rate back to trend were the result of government policy, then so were the world-beating Peruvian deaths .
“Those who criticize Sweden also need to explain Peru, where despite what was likely the world’s earliest, harshest, most mask-wearing lockdown, COVID mortality per capita is the highest in the world,…” I had a Covid-19 test in Fl in June 2020. I was wearing my mask upside down (I’m 84 yrs old) the tech WARNED me, told me how to pinch the top for the nose and to be careful “… material gloves and masks are DANGEROUS if not properly used and cleaned because ‘they become carriers of the disease. You could even bring it home. Why is it we hear 100,000 times “Must Wear Mask” and not even one time “Caution Improper use may cause disastrous results”.?
Sorry Doc, I don’t see your Sweden vs Norway comparison as valid. All it proves is covid will get you sooner or it will get you later. Hole up in your bunker and you drastically reduce the risk of getting it but step out into a world that has been destroyed economically and, shazam, you get covid later than otherwise, assuming you haven’t committed suicide in the meantime.
The lockdowns were meant to temporarily flatten the curve to give hospitals etc. breathing space not prevent the eventual spread. Now taken on a life of their own.
Personally, I don’t care if you disagree with the Great Barrington Declaration or approve of Fauci or whoever, science like politics has shown it is eminently corruptible. Cui Bono?
The choices we have been presented with – stay home or you’ll kill people – are false choices. I come down closer to the Barrington group vs others. I live in Illinois, one of the states that has not done a particularly good job of protecting the elderly (not the disaster NY and NJ were, but still bad). We need to protect the vulnerable, but as others have noted, the risk is very small for people under the age of 55. 80% of the deaths are in people over the age of 65. The median age of COVID deaths in the US: 78. Median lifespan? 78.
COVID does kill people, but so do a thousand other things, including poverty, stress and unemployment. I live in Chicago and the attendance rate for online learning is in the 40-70% range, at the low end for the schools with the lowest incomes. These kids will continue to fall further behind. Meanwhile, other countries not going through an election have had kids in school since early spring with no discernable impact on the death rate. I was on the phone earlier with someone in Zurich and his kids went back to school this spring and again this fall. Older kids wear masks. All teachers wear masks. And for the kids, life goes on and the parents can work. Not so much here.
Those of us who can work from home and send our kids to private schools that are in session will continue to win while the less fortunate are pushed ever further down.
The proposal to protect the most vulnerable and let herd immunity grow as the rest of the community gets infected and (hopefully) gets over it without harm ignores the elementary fact that the virus is passed on quite efficiently by persons without symptoms, so the most vulnerable would likely take a big hit.
I know medical and other folks will disagree but I feel all disease is due to dis ease in the world . Like any natural catastrophe, it is a natural way to clean the environment, nature, including people, animals and plants. This dis ease in the world, particularly stemming from humans, can and will only be stemmed when we see each human on the earth as valuable as ourselves. This is a time when all must look inside themselves and see if they are in unity with each other. Worldwide. Not just our little selves, family , community. Survival of the planet depends on this.
You had me until”when all must look inside themselves”. There will be plenty of time for philosophical musings when the dying has stopped. And this was an excellent article except for quoting Dr. Fauci as a Doctor and an expert. The man waited 80 years for his shot at the limelight and salivates at each camera trained upon him as he contradicts himself yet again to gain even more camera time. Put him in a closet and toss away the key please!
Nice summary of the vaccine developments….watching this space closely for an effective vaccine (which will move at the speed of science for sure).
Doc gumshoe
If a future column addresses Covid severity, may I recommend that Doc G. take a look at the work of @sanchak74 on Twitter?
Since February, I have been following his use of only published data to argue that the serious sequellae of a Covid infection result, not from the virus, but from the virus enabling a secondary infection of anaerobic bacteria (eg. Prevotella) in a way similar to the Epstein Barr virus operates in Lemierre’s Disease.
I’m a chemist, not a bacteriologist, but to my eyes, he has been very conservative and logical in his proposals and I have yet to find an unsubstantiated claim in his hypothesis.
IF he is correct, the glitter of a $B viral vaccine may be blinding medicine from a much simpler solution.