This morning my wife phoned to tell me that she had stopped in at a little local store where she occasionally shops. She learned that the owner had just come down with COVID. She was concerned, because she had been in the store a couple of days ago, been close to the owner, and purchased several items which the owner had certainly handled.
My optimistic persona came to the fore and told her not to worry. She would most likely not get COVID, and if she did, it would almost certainly be a very mild case. But she patiently pointed out to me that both of us (particularly Yours Truly!) are of an age that is more vulnerable to serious COVID symptoms, and that we have upcoming plans that we don’t want to mess up. And also that we can’t rule out long COVID, which progresses from being a nuisance to being a serious problem.
Therefore, said she to me, Wear Your Mask When You Are in a Public Indoor Space. Docile Doc Gumshoe assented.
So, despite the fact that the World Health Organization declared that the global COVID-19 emergency was over, COVID is still with us, and will continue to be with us for … who knows how long?
Yes, on Friday, May 5th, the WHO director-general, Tedros Adhanom Ghebreyesus said, “It is with great hope that I declare COVID-19 over as a global health emergency.” But Dr Maria Van Kerkhove, WHO’s technical lead on COVID, said the organization wanted to be as clear as possible, knowing that people would wonder how to think about the pandemic going forward.
“The emergency is over, but COVID is not,” she said.
As we all surely know, the US lifted the COVID emergency on May 11th. At the start of the pandemic, Dr Anthony Fauci warned of a worst-case scenario in which the US would experience a million deaths due to COVID. His worst-case scenario was exceeded; total US COVID deaths to date are more than 1.1 million. It’s estimated that about 94% of the US population has experienced at least one COVID infection. According to WHO, a large majority – perhaps three-quarters – of all the planetary populace has had a COVID infection.
In middle- and high-income countries, it’s estimated that somewhere around 70% of the populations had been vaccinated by the end of 2021. At that time, only about 3% of people in low-income countries had been vaccinated. That number in low-income countries has since grown to 23%,
As a cause of death in the US, COVID has receded from the top three in each of the first three years of the pandemic (2020-2022) to the seventh in 2023. This is certainly because, between vaccination and immunity from having contracted the disease, the US population is much less susceptible to COVID.
Another way of looking at the impact of COVID is attempting an accurate estimate of the number of excess deaths. What the statisticians mean by that is the number of deaths during a specific period of time that exceeds normal death rate during that same period. When the statisticians come up with such a number, they look for a cause – what happened during that period that might account for the out-of-pattern number of deaths. Sometimes that cause is a single rare event – the 1970 tsunami in Bangladesh that killed between 300,000 and half a million people in the course of a few days.
In the past three-plus years, the excess global mortality has almost certainly been due to COVID. The number of excess deaths began to climb markedly in 2020, as the COVID pandemic took off, and these numbers have not declined significantly. Currently, according to the database maintained by The Economist, excess deaths are running at about 11,000 per day. The number has fluctuated between 8,000 and 15,000 per day during the past 12 months. The current predicted number for annual excess deaths is about 4 million; this is slightly higher than the estimated number for 2020, as the pandemic was taking off.
In spite of the marked disparities in the vaccination rates between low-income and higher-income nations, their excess mortality rates were similar. Initially, high-income nations were faring decidedly worse than low-income nations, perhaps because a higher fraction of their populations consisted of older folks with underlying conditions, whereas the populations of the poorer nations were younger and therefore less vulnerable. However, as more of the people in the higher-income parts of the world got vaccinated, the excess mortality rates between the lower and higher income cohorts evened out. Lower income nations have already had as much excess mortality in 2023 as in all of 2020, while excess mortality in higher-income parts has declined.
The current COVID -19 picture in the US
An indication of the COVID status in the US and globally is that my preferred source of information, the Johns Hopkins COVID tracker, ceased operation on the 10th of March this year. On one screen it displayed new cases and deaths, not only in the US, but globally, as well as the cumulative totals. Within any nation, one could zoom in on a district or even a single city, and the data would appear. Why has it quit operating? My guess is that it took a huge amount of work, gathering all the data and inputting it to a single quasi-magic screen. And as COVID-19 waned, they figured it just wasn’t worth the effort.
Happily, the CDC is still providing relatively current data for the US, at least. As of 9 May 2023, there were 77,294 reported new cases of COVID per week. The number of deaths due to COVID were 1,109 per week, and there were 1,333 new hospital admissions per week. Based on data reported by the CDC in April, the week over week decline in the number of new cases was 17.3%. The decline in deaths was 14.9%, and the decline in hospitalizations was 25.2%.
May I point out that we’re looking week-over-week declines in new cases, deaths, and hospitalizations, and that these are declines taking place over a very short period. Based on those, we can’t be sure of the long-term trends. We need to look at longer-term data.
These numbers need to be compared with the numbers of new cases and deaths during, for example, the peaks in January of 2022, when the daily new cases rate reached more than 800,000, and there were more than 2,500 COVID deaths per day – not per week, per day! According to my calculations, the current new case rate is approximately 1.5% of what the new case rate was when COVID-19 was raging at its peak.
Is that good news? Can we take that as a strong indication that the pandemic is really on the way out? For the present, there’s no doubt that it’s excellent news – far fewer cases, far fewer deaths.
Here’s a look at the COVID death toll over the past three years. According to the CDC, there were 1,131,729 deaths attributed to COVID-19 as of May 3, 2023.
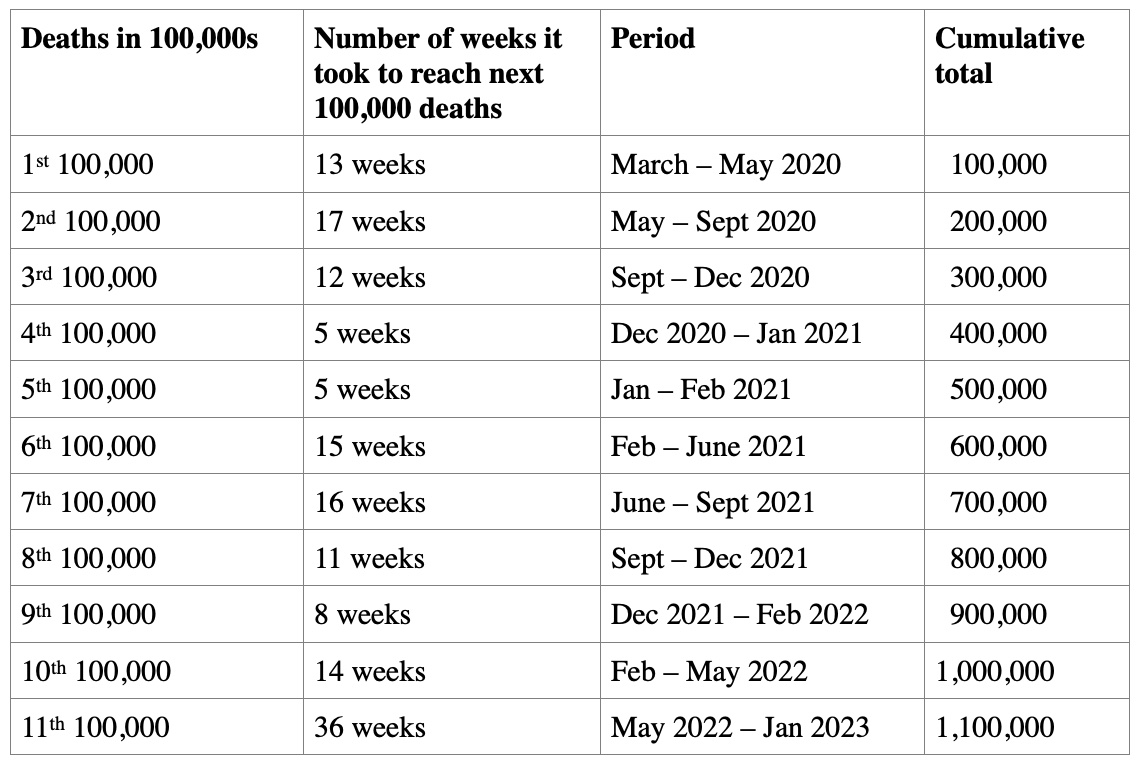
The table highlights the stark differences between the periods when the coronavirus was raging virtually uncontrolled, in the winter months of 2020 – 2021, and the distinct slowing in the spring and summer of 2021, when vaccines became available for adults in the US. No, we can’t attribute the decline solely to the availability of vaccines, but it looks like more than a coincidence. And then, in the fall and winter of 2021 going into 2022, we had those variants – Delta and Omicron, if you remember.
It’s hard to predict how long it will take for the next 100,000 deaths to occur. One hears statements that the US is still experiencing about a thousand COVID deaths per week. At that rate, it would take a couple of years to reach the 1,200,000 deaths marker, and that only if the death rate continued at that present pace. Which, all things considered, seems unlikely. Based on the very high percentage of people who have already had COVID, and on the respectably high percentage that have been vaccinated, we could expect the death rate to diminish significantly.
"reveal" emails? If not,
just click here...
There are certainly reasons to think that, even if there is an increase in the new case rate, it won’t be anywhere nearly as steep as some of the previous peaks. The reasons for this optimistic view is that at this point in the US almost everyone has either had COVID or been vaccinated, or both. The number of individuals with no immunity is very small.
Of course, the coronavirus has the capacity to reinfect persons who supposedly have robust immune levels, especially if the immunity came from infection from an earlier variant, or from vaccination with an earlier version of the vaccine. (Parenthetical note: at 4:00 PM today I am getting my second shot of the bi-valent booster, further evidence that I continue to be cautious.)
The NY Times interviewed several experts for guidance about how we as individuals should behave to protect ourselves and people with whom we come into contact. Dr Robert Wachter, chair of the department of medicine at the University of California, San Francisco, continues to wear a mask in most crowded indoor settings such as on an airplane or in a museum. However, when he needs to pop into a store, he does not wear a mask.
Dr Caitlin Rivers, an assistant professor at the Johns Hopkins Bloomberg School of Public Health, said she had stopped wearing a mask at the grocery store or in the office, but she still puts one on in public transportation.
Dr Krutika Kuppali, an infectious disease specialist tests herself before going to big indoor gatherings. “I think we have to do what we can to mitigate risk, not only for ourselves, but we also live in a community.”
These individuals expressed concern lest a new, more infectious variant should emerge. Currently, the Omicron subvariant labeled XBB.1.5 accounts for about 78% of COVID-19 cases in the US. This subvariant has been the dominant strain the US since the beginning of 2023. It is considered to be the most transmissible strain of the virus so far. Meanwhile, experts are still learning about several newer Omicron strains circulating in the US, none of which are causing more than 10% of infections. These include BF.7, XBB.1.16, XBB.1.9.1, BN.1, BF.11, and others.
Dr Kuppali said she was paying close attention to XBB.1.16, also known as Arcturus, which is driving a surge in India. That variant brings a different symptom not previously associated with COVID: conjunctivitis, commonly known as pink eye.
Dr Rivers, on the other hand, is focusing her attention on another variant, XBB.1.9.1, which currently accounts for about 8% of infections in the US. She expects the cases to start rising as the weather warms.
Concerns about long COVID
Dr Robert Wachter was quoted as follows:
“Unlike the way I felt two or three years ago, I have no fear that I’m going to die of this thing But I think long COVID is very real. My wife has a mild version of it, so I see it up close and personal.”
Concerns about long COVID are on the rise. I was personally surprised at the prevalence of long COVID, which is defined as symptoms lasting three months or longer after first having been infected with the coronavirus. In the US, about 7.5% of adults – one in thirteen – have long COVID symptoms.
The estimates for the global prevalence of long COVID are startling. Based on the number of documented cases of COVID-19 on the planet, which comes to 651 million, and the estimated incidence of long COVID as 10%, at least 65 million individuals around the world have long COVID. The number may be much higher due to many undocumented cases. The incidence is estimated at 10–30% of non-hospitalized cases, 50–70% of hospitalized cases, and 10–12% of vaccinated cases.
The symptoms of long COVID are not much different from the symptoms of an acute infection, the most common being a cough, fatigue, shortness of breath, muscle and joint pain, problems getting a good night’s sleep, loss of smell and taste, a low mood and depression, and anxiety.
WHO has adopted International Classification of Diseases code U09.9 for the definition of long COVID as the onset of new symptoms after the original bout of illness or positive COVID test. In addition to the symptoms listed above, WHO lists fatigue with or without exertion, glucose intolerance, multisystem inflammatory syndrome, postural orthostatic tachycardia, and peripheral neuropathy.
Long COVID tends to affect people in their fifties about three times more often than people in their eighties. (I consider that excellent news!) Women are somewhat more likely to be affected by long COVID than men. Hispanic adults have a significantly higher likelihood of being affected, about 9%, than White, Black, or Asian adults.
According to WHO, long COVID is defined as the continuation or development of new symptoms three months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least two months, with no other explanation. The definition does not point out that in long COVID the acute phase is over. Patients are no longer experiencing the immediate effects of infection with the coronavirus. There is not enough active coronavirus in their systems to elicit a positive response on the test. But while the coronavirus was active, it probably inflicted long-lasting harms on the patients’ physiologic function, whether respiratory, cardiac, digestive, or other.
In spite of the unfortunate fact that long COVID is fairly common, the health-care world has given it relatively little notice. The key phrase in the WHO definition above is “with no other explanation.”
A recent article in the New England Journal of Medicine (2023 May 9.doi:10.1056 NEJMp2304550) contrasts the impressive concerted efforts that were made by government and the health-care community to address the challenges of the COVID pandemic with the lack of support and lack of attention that long COVID has attracted. The authors, J. Z.Nikolich and C. J. Rosen, note that the clinical presentations of long COVID are highly variable, and there is no well-accepted definition of the syndrome. As a result, there is no evidence-based treatment for long COVID, however it is defined.
As noted above, there is no clear definition of long COVID. A fundamental assumption is that if some COVID symptoms return after the initial confirmation that the patient has been infected with the coronavirus (and recovered from the acute symptoms), that patient has “long COVID.” The usual criterion for making that assumption is that the initial infection took place two months prior to making the long COVID diagnosis. This does not clearly define long COVID, because some patients develop COVID-like symptoms without having initially tested positive for the coronavirus. Treatment strategies for persons with long COVID do not focus on eliminating the virus, but on managing the lingering symptoms. In a sense, it is a retreat from current medical practice, which focuses on finding and treating the cause of a disease or condition, and returning to a less sophisticated form of medicine, which focuses on the symptoms only.
Patients with long COVID sometimes feel that they are not getting the full attention and respect of providers, who sometimes adopt the attitude that their symptoms are psychosomatic. In other words, that their symptoms are mostly caused by anxiety or stress, and beyond the capacity of a regular MD to treat. No matter how carefully the provider communicates this view to the patient, what the patient hears is that the provider thinks “it’s all in my head, and they can’t do anything for me.”
Although some clinics for the treatment of long COVID have been established, the majority of affected patients are followed either by primary care providers, or – depending on their dominant symptoms – by various specialists. Referrals to subspecialists such as cardiologists, pulmonologists, and neurologists are common but these often lead to even greater delays and frustration at all levels. Primary care providers feel the brunt of that frustration at their inability to help beyond deploying simple strategies, such as exercise or nutritional supplementation, that are used as preventive measures for healthy people.
The National Institutes of Health has launched an initiative to identify and define the clinical spectrum and pathophysiology of long COVID, to determine its natural history and prevalence, and to characterize the way in which the coronavirus causes significant symptoms after the acute disease phase. It has been named the Researching COVID to Enhance Recovery (RECOVER) initiative, and it has a network of enrollment sites in 33 states, the District of Columbia, and Puerto Rico. It is working with community partners to enroll 12,000 participants.
The lack of attention to long COVID is understandable. From the beginning of the pandemic, the focus has been on attempting to control the spread of the disease, and treating the patients with the most severe symptoms and those at highest risk of hospitalization and death. However, long COVID is attracting increased attention. For example, just about a week ago, on May 9th, Anna C. Eshoo, a House member from California and a Ranking Member of the Subcommittee on Health, wrote a letter to Dr Lawrence A. Tabak, Director of NIH, pointing out that the efforts of the RECOVER initiative are far from being realized.
Her letter said as follows:
“More than three years into the pandemic, the number of Americans reporting chronic Long Covid continues to rise, with almost 20 million currently reporting symptoms, and 4 million unable to work because of their symptoms. There’s no standard protocol for diagnosing or treating Long Covid or a deeper understanding of the illness and its causes. To date, the NIH has not signed a single patient up for a clinical trial to test Long Covid treatments or set a specific date to begin enrollment, despite telling Members of Congress that clinical trials would begin in the fall of 2022. Instead, NIH has obligated over $918 million of its RECOVER funding to long-term research studies and data analytics that have not brought much-needed relief to Long Covid patients.”
It does appear that as the acute phase of the pandemic is tapering down, the health-care community has a bit more capacity to focus on the long-term effects. We look forward to progress on that front.
Why does heart inflammation after COVID vaccination particularly affect young males?
Jumping ahead to the conclusion, that particular question remains unanswered. After extensive research, experts have to some degree figured out the specifics of the condition, but not why it especially affects young males.
Heart inflammation after vaccination tends to resolve very quickly, and cases are very rare. The group at highest risk consists of teen-age boys. In this group, heart inflammation, called myocarditis, occurred in 26.7 of 100,000 cases receiving the second vaccine dose, or 0.0267%. In contrast, myocarditis occurs in 59 of 100,000 actual cases of COVID-19. The myocarditis cases after vaccination also tend to be significantly milder than myocarditis occurring due to other causes.
There were several theories as to why myocarditis was occurring after vaccination. The most obvious were that the vaccine recipient mounted an allergic response to the vaccine, or that the vaccine triggered an autoimmune response in which the recipients’ immune system mistakenly attacked the body’s own healthy tissue.
Either of these would have been very difficult to treat, with a risk of significant adverse effects. Instead, in a study that investigated the phenomenon in 23 patients, researchers found signs that the myocarditis was inflammation-induced. It did not appear to be an autoimmune response, but a response specifically to the vaccine. (Barmada A., Science Immunology, 5 May 2023 8; 83; DOI: 10.1126/sciimmunol.adh345).
Each of the leading possibilities as to the essential cause of myocarditis after vaccination were thoroughly explored. Researchers did not detect greater antibody levels in patients who had developed myocarditis than in a control group, suggesting that the heart condition was not caused by vaccine-induced antibodies. They also found no signs of immune cells that looked like the pattern typically seen in an autoimmune response. That finding is valuable in the sense that if the condition was the result of an autoimmune response, patients would have to be given higher doses of steroids, or need to take them for longer periods, risking more side effects.
What they did find were elevated levels of inflammatory proteins such as interleukin 15, and also a proliferation of tissue-damaging immune cells.
A measure that might reduce the incidence of this already rare reaction might be to allow a longer interval between the first and second doses of the vaccine, allowing the immune system to calm down.
As to why it preferentially affects teen-age boys, my speculative answer might be that the particular population most affected by post-vaccine myocarditis also happens to have a particularly active immune system.
In any case, the very low incidence of post-vaccination myocarditis and very mild harm caused by this rare condition in no way presents a valid reason to avoid vaccination. Postpone the second dose, yes; skip it altogether, no.
A small addendum to “Weight and Waistline Worries”
You may remember that in that piece, which posted just a couple of weeks ago (May 3rd, to be precise) we discussed the roles of glucagon-like peptide and semaglutide in combating obesity. In case you were on vacation on a tropical isle and missed it, here’s a bit of background from that piece:
“…A diet high in fats inhibits the function of the hormone that tells us that we don’t need to eat any more.
How can this be remedied? Fortunately, there is another hormone in the picture. It’s called glucagon-like peptide, abbreviated as GLP-1. GLP-1 functions as an agonist of leptin (agonist being the opposite of antagonist), boosting its function in signaling satiation. Leptin communicates to the sensory areas of the brain the sensation that we have had quite enough to eat, thank you. GLP-1 also stimulates the production of insulin and brings down the levels of HbA1c, which is an indicator of how much glucose is bound to the hemoglobin in our bloodstream.
Semaglutide, a peptide that almost duplicates GLP-1, has been developed and brought to market by Novo-Nordisk. It was first marketed as Ozempic for the treatment of Type 2 diabetes, and has been FDA-approved for treatment of T2DM since 2017.
In 2021, Novo Nordisk won FDA approval for semaglutide as an anti-obesity medication, and began marketing it under the name Wegovy.”
A study published just a few days ago points to another effect of semaglutide/Wegovy. (De Barra C. Obesity. 9 May 2023 https://doi.org/10.1002/oby.23772 ) In obese individuals, the NK function is diminished. But in this clinical trial, Wegovy was shown to restore natural killer cell function in 20 obese subjects.
Natural killer (NK) cells are a type of white blood cell that kills viruses and cancer cells. They come from the same family as T and B cells, but differ in that they unleash their destructive power without having to be primed or activated first. While NK cell activity is actually enhanced in the early stages of weight gain, the killer cells in the peripheral circulation lose their cancer-killing ability over time if the weight gain continues. This is probably one of the mechanisms that explain why more obese persons develop cancer than those who have been able to keep off the excess weight.
The subjects in the study were given once-a-week doses of semaglutide/Wegovy at the typical starting dose of 0.25 mg and working up to 1.00 mg over the six month study period. At the end of the study, the study subjects had not experienced an increase in the total number of NK cells, but the NK cells were producing greater numbers of cytokines that specifically attack cancer cells.
A natural assumption would be that what improved the NK cells’ activity was the weight loss that the study subjects experienced. But mathematical analysis of the findings suggested that weight loss was not the cause. There was no statistical relationship between weight loss and improvements in the various components of NK cell metabolism and cytokine production. Furthermore, exposing NK cells to semaglutide/Wegovy in a Petri dish resulted in the same boosting in their cancer-killing capacity.
The results of this small and limited study certainly do not suggest that Wegovy should be employed as an anti-cancer drug, but it does point to further research on ways of enhancing our own defenses against cancer.
Since Wegovy soared to blockbuster status due to its weight-loss effectiveness, the drug has been publicly adopted by celebrities like Elon Musk, which has led to a rush by great numbers of the non-obese-but-perhaps-a-tiny-bit-overweight population to get Wegovy. And, as a consequence, shortages!
* * * * * * *
I would like to think that there will come a time when COVID really and truly fades into the background of minor health concerns. We’ll just have to wait and see.
Stay well, everybody! Enjoy this wonderful May weather we’re having, around here anyway! Thanks for all comments! Best, Michael Jorrin (aka Doc Gumshoe)
[ed note: Michael Jorrin, who I dubbed “Doc Gumshoe” many years ago, is a longtime medical writer (not a doctor) and shares his commentary with Gumshoe readers once or twice a month. He does not generally write about the investment prospects of topics he covers, but has agreed to our trading restrictions. Past Doc Gumshoe columns are available here.]
So…why does the US have the highest Covid death rate? Something doesn’t seem right…
Mostly because the threat from the coronavirus was greatly underestimated, and in some cases, disparaged as “no big deal.”
Very informative! Was wondering whether I should have a fifth Covid shot, and reading this makes me think I should.
I would think long and hard about that before you act.
why”
because its not needed that’s why and not for everyone
Pfizer recommends a fifth shot for those who didn’t die from the first 4.
Good one!
lets stick to stocks. the plandemic is over. many of us think the shots are more dangerous than the flu.
Interview Dr Judy Mikovitz and then have another chat with us…. she will help you understand the science.
It’s Mikovits and I doubt that she will help.
She has been thoroughly discredited.
Thanks Doc, great work. Unfortunately, I am compromised so I must keep up with the news and be careful even though the exalted ones state that it is over. The shot was not even a real vaccine by the CDC’s own definition. I still find it amusing that all are still not allowed to call it “The China Virus” or post it as such. Spain was not so lucky as The “Spanish Flu” did not even originate there but they got blamed for it!
Long COVID for some can be very debilitating and even so severe it puts you on total disability. The wife on an acquaintance who was a busy family physician has long COVID and has severe weakness and breathing problems that she had to quit and go on total disability. The May 13, 23 WSJ had an article on long COVID and mentioned a support group named React19 which has a website an is on FB.
It is a big boom–weight loss drugs–but they are delivered by injection. Pfizer is in a late stage phase of an oral drug that appears to be as good and Pfizer is a fortress in drug development, pays a nice dividend, and in my opinion, undervalued. Check it your self.
I have an anti vaxx friend who quit his job due to side effects from the jabs. He went through at least four medical practitioners/institutions for tests over two or three months. In the end, it turned out that drinking around seven cups of coffee a day was the problem. He stopped cold turkey (after thinking tea was the ideal replacement) and went back to work after his “vaxx injuries” cleared up.
Dying from Covid is not the same as dying with a few virions of Covid, but the numbers combined all deaths where Covid was detectable, and the detection equipment was turned up 10 to 100 times recommended setting. Look it up.
Doc Gumshoe, check out frontline doctors https://americasfrontlinedoctors.org/about-us and father of nanoparticle mRNA research, Dr. Robert Malone and https://worldcouncilforhealth.org/multimedia/robert-malone-health-conference-ireland/
Just Fyi Other deaths are still being reported as covid deaths . Its a simple form a doctor fills out when someone dies that lists a diagnosis.
It is not very scientific . When a patient dies
A doctor has to fill out a death certificate time date of death and released to funeral home coroner etc. and notification of family.
But its a government form to let the govt know that they do not need to pay for that soc security medicare etc etc. and county division of assets /taxes of those based on wills trusts etc. Is has a diagnosis cause of death which
Is only determined by what supposed diagnosis is in the patients chart or old history. For example someone dies and obviosly their heart stopped, they stopped breathing, and their brain died. Which one caused their death or what caused them to stop ? Usually only an autopsy is reliable and not done very often.
Generally the doc is just trying to get the form filled out listing any diagnosis in the chart. The doc doesn’t have to provide proof of what caused the death and
doesn’t get extra pay so they just fill in whatever is convenient. So anyone with a recent dx of covid gets covid19 because its shorter and easier to write than myocardial infarction of the blank blank blank. The pharmaceutical companies use this to push their drugs. Allot of times the primary care will be asked to fill it out after the fact and has not seen the patient because they dont go to the hospital anymore they stay in there clinic.
We arent admitting very many patients with covid any more 2-3 in 6 months but many patient with surgeries fractures uti that also have a positive covid test which stays positive for 10 days. If a patient dies at home the provider provides a probable cause without even seeing the patient.
The bottom line is , information on cause of death statistics is very very poor and can be used for whatever narrative .
I have a friend who determined that the fact that I got Covid last year, as did he, showed that the shots really weren’t any good. The fact is that I got a rather mild case, with zero respiratory symptoms. He, with no shots, ended up in the hospital with a respirator.
My doctor daughter says that is what the shots are designed to to do: which was greatly reduce the illness. And I am in what is considered a high risk group.
have a friend that had 3 shots and then lost his life we think the shots they say covid
Doc Gumshoe, I think you should show the tables showing death rates per age and per comorbidity and also which comorbidities have the biggest effect.That lets people realize that age and comorbidity and race play an enormous role.
The mainstream media and WHO, CDC and other tend not to show this.
I am double vaxxed and 72 and had 3 diagnosed infections so I am not an unbeliever. I had and have very little fear for my grandchildren to get very sick.
Let’s get all the facts out there.
I would like to, but I’m not sure I can get all the necessary data.
covid shot more dangerous than the covid, in our 70ies wife and myself no shots and covid twice like a cold for us. And two of friends had major complications from shot, it is a personal choice and the shot is something we would never do and way to much info out there now.
A recent study of 51,000 Cleveland Clinic employees stated in its next to last paragraph, “The association of increased risk of COVID-19 with higher numbers of prior vaccine doses was
unexpected.”
Here is a link to the study which was peer-reviewed and published in the medical journal Medrxiv: https://www.medrxiv.org/content/10.1101/2022.12.17.22283625v5
Earlier this month a peer-reviewed article was published in the medical journal Cureus entitled Estimation of Excess Mortality in Germany During 2020-2022. In the article, below Figure 8, the authors found the “hypothesis of a decrease in excess mortality with an increasing number of vaccinated persons is not correct. During periods when many people were vaccinated, excess mortality seems to have increased more strongly compared to the same periods in the previous pandemic year.”
Here is a link to the article:
https://www.cureus.com/articles/149410-estimation-of-excess-mortality-in-germany-during-2020-2022#!/
The bottom line is the MRNA Covid-19 vaccines are not effective and are not safe. Instead, they should be avoided.
Jsut curious about those doctors who occasionally wear masks. What kind of masks do they wear in public and why?